KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 35(2); 2020 > Article
-
Original Article
Therapeutic Effects of Prolonged Release Melatonin (Circadin®) in Patients with Overactive Bladder and Chronic Insomnia in More Than 55 Years Old - Min Jung Park, Seon Young Seo, Hyun Jun Park, Jih Hoon Park, Mi Young Lim, Nam Cheol Park
-
Kosin Medical Journal 2020;35(2):101-113.
DOI: https://doi.org/10.7180/kmj.2020.35.2.101
Published online: December 31, 2020
1The Korea Institute for Public Sperm Bank, Busan, Korea
2Department of Urology, Pusan National University School of Medicine, Busan, Korea
- Corresponding Author: Nam Cheol Park, Department of Urology, Pusan National University School of Medicine, 179, Gudeok-ro, Seo-gu, Busan 49241, Korea, Tel: +82-51-240-7349, Fax: +82-51-247-5443, E-mail: pnc@pusan.ac.kr
• Received: April 14, 2020 • Revised: July 28, 2020 • Accepted: September 28, 2020
Copyright © 2020 by Korean Association of Medical Journal Editors
Articles published in Kosin Medical Journal are open-access, distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,165 Views
- 22 Download
- 1 Crossref
Abstract
-
Objectives
- Bladder storage symptoms including nocturia is the most common cause of sleep disturbance in all age groups. Sleep disturbance is also a main cause of nocturia so that sleep recovery can clinically improve nocturia. Melatonin has main action to induce sleep and additional effects of smooth muscle relaxation, free radical scavenging, anti-inflammation, et cetera. This study was evaluated the improvement of sleep quality after administrating prolonged-release melatonin in elderly patients with overactive bladder and chronic insomnia.
-
Methods
- This clinical trial was performed with a randomized single open study. Thirty-seven patients with overactive bladder and chronic insomnia were initially enrolled in this study. After 4 or 12 weeks treating with 2 mg of prolonged-release melatonin, clinical outcomes were evaluated with OABSS, IPSS, PSQI and WHO 5 well-being index.
-
Results
- Of the 37 patients, 34 (91.9%) were included in the ITT group and 26 (76.5%) in the PP group. In the primary outcome of PP group, significant improvements were observed in total OABSS and nocturia frequencies at 12 weeks, respectively. Secondary outcome measurement including in voiding, storage symptoms, and total IPSS scores showed the improvement at 4 and 12 weeks and in total and sleep quality PSQI scores at 12 weeks, and in quality of life scores of the WHO 5 well-being index at 12 weeks. Only one (3.8%) adverse event was observed.
-
Conclusions
- These results suggest clearly that prolonged-release melatonin in elderly patients with overactive bladder and chronic insomnia has the potential to control concomitant voiding and sleep difficulty.
- Study design
- This clinical trial was performed with a pilot randomized non-placebo controlled single center registry-based prospective clinical trial as investigator intended post-marketing testing in accordance with the Good Clinical Practices standards and in conformity with the ethical principles set out in the Declaration of Helsinki. Demographic characteristic, medical history, presenting symptoms, and variety of treatment outcome data were collected by trained nurses using a standardized case report form at each site.
- Subject screening and clinical outcomes during 12 weeks treating with Circadin® were evaluated with overactive bladder symptom score (OABSS), international prostate symptom score (IPSS), Pittsburgh sleep index (PSQI) and WHO 5 well-being index. For the assessment of sleep quality, a specialist in sleep disorders was recommended the PSQI which was a self-report questionnaire.7–11 Screening for subject suitability was performed with OABSS, IPSS and PSQI with pretrial wash-out at least 4 weeks before administration of the investigational product on visit 1. At visit 2, 3 and 4, OABSS, IPSS and PSQI were reviewed with the subject’s diary to be conducted at baseline and after 4 and 12 weeks of treatment. At visit 2 and 4, WHO 5 well-being index were also evaluated with checking physical examination, vital signs, laboratory test and echocardiography. At visit 4 after medication, adverse event was evaluated (Fig. 1). Randomization numbers were given to patients who were judged to be suitable for the clinical trial.
- Subjects
- The subject criteria to be enrolled in the screening test were OABSS scale 2 ≥ 2, OABSS scale 3 ≥ 2, and PSQI ≥ 5. Inclusion criteria in this study are adult male more than 55 years, history of OAB recent 3 months or more, total score 3 < and Q2 2 < on overactive bladder symptom score, patient with chronic insomnia and completed patient informed consent prior to clinical trial. The exclusion criteria are as follows; clinically significant bladder outlet obstruction, patient with overactive bladder due to neuropathic causes, patient with bladder stone, interstitial cystitis, active urinary tract infection, patient with previous or current pelvic organ cancer, patient with secondary insomnia due to obstructive sleep apnea, chronic pain or restless legs syndrome, case with irregular sleep pattern, shift-worker, case to have contraindicated medication during clinical trial, patient with clinically serious liver or kidney disease by investigator decision making, participant of other clinical trial, and case not to visit according to time line of clinical trial. Concomitant medications to be prohibited are alpha blocker, 5-alpha reductase inhibitor, anticholinergic agents, antimuscarinic agents, herbal medications for voiding difficulty or overactive bladder, cimetidine, adrenalin agonist and antagonist, opioid agonist and antagonist, antidepressant, prostaglandin inhibitor, benzodiazepine and non-benzodiazepine hypnotics, imipramine, thioridazine, methoxsalen, fluvoxamine, CYP3A4 inhibitors including ritonavir, saquinavir, ketoconazole, itraconazole, erythromycin, Clarithromycin, grapefruit juice, voriconazole, indinavir and nelfinavir, CYP1A2 inhibitor including quinolone, CYP1A2 inducing agents including rifampicin and carbamazepine.
- Ethics statement
- The study protocol was approved by the Institutional Review Board at Pusan National Hospital (PNUH IRB No. D-1704-002-064 (Apr. 27, 2017) as well as Korea Food and Drug Administration (KFDA) Approval No. 31223 (March 08, 2017). Informed consent was obtained by all subjects when they were enrolled.
- Investigational drug
- Circadin® (Kuhnil Pharm, Seoul, Korea), originally developed by H. Lundbeck A/S (Copenhagen, Denmark), is a prolonged-release medicine of 8–10 hours to be possible full night melatonin coverage.6 Dosage and administration are 2 mg of prolonged-release melatonin on 1–2 hours before everyday bedtime.
- Efficacy assessments
- Primary end point for efficacy outcome assessments were changes of OABSS with total score and Q2 (nocturia frequency) score from baseline to 4 and 12 weeks. Secondary end points included changes of IPSS with total score, voiding symptom score and storage symptom score, PSQI total score, PSQI Q9 score from baseline to 4 and 12 weeks, changes of WHO 5 well-being Index (1998 version) for evaluating quality of life, total score, on baseline and after 12 weeks of treatment.
- Safety evaluation
- Safety evaluation at weeks 4 and 12 included physical examination, vital signs, laboratory test, echocardiography and findings. Adverse events were assessed for patients who took at least 1 dose of Circadin®. Adverse events reported in response to general and non-specific inquiry survey by the researcher or self-reported by the patient were described with severity at each visit according to the World Health Organization (WHO) Adverse Reactions Terminology (WHOART) system organ classes. Adverse drug reactions related to the investigational product were compared using the same method.
- Statistical analysis
- The intention-to-treat (ITT) analysis was conducted for all randomized subjects to analysis of all subjects initially enrolled in a clinical trial. The per-protocol (PP) population was defined as those subjects in the ITT population who had completed the visit and for whom there were no serious protocol deviations. In this study of PP group, the treatment efficacy was determined by comparing primary and secondary outcome measures at the end of each treatment.
- According to the standards of a per-protocol analysis, sample size was calculated with 37 participants by G Power 3.1, at least 34 participants to be recruited plus 10% unfaithful responders. Statistical analysis of data from inquiry survey was performed by paired t-test. Changes from baseline in continuous safety variables including vital signs, laboratory analysis, echocardiographic finding and were evaluated by ANOVA. Efficacy measured in ITT and PP groups included the mean ± SD changes at 4 and 12 weeks from baseline. Statistical significance was accepted for P values of < 0.05.
MATERIALS AND METHODS
- Demographics and Baseline Characteristics
- The patients in this study were recruited consecutively and evaluated prospectively for 1 year between July 2017 and August 2018. Initially, eligible patients had minimal 4 weeks and maximally up to 12 weeks treatment-free run-in period and then were checked for adequacy for inclusion. Thirty seven patients were screened in this study. A total of 34 patients were enrolled in the ITT group. Overall, 26 patients (76.5%) of these were completed the study in the PP group. The demographics and baseline characteristics of the volunteers in the ITT and PP groups are shown Table 1. Data from two groups were used to analyze efficacy parameters. Mean patient age in the ITT and PP groups were 69.5 ± 7.7 and 69.8 ± 7.7 years, respectively. At baseline, no clinically or statistically meaningful difference was found between the two groups with respect to demographic or clinical variables.
- Efficacy outcomes
- Data on the effectiveness of this clinical trial were conducted by the ITT group which enrolled efficacy assessment after receiving at least one clinical treatment. The PP group followed visitors for 12 weeks without major violations among the ITT group, the targeted 26 patients with a compliance rate of 76.5% was included in the PP group. Analysis of primary and secondary efficacy endpoints was only measured on the PP group.
- Primary efficacy outcome
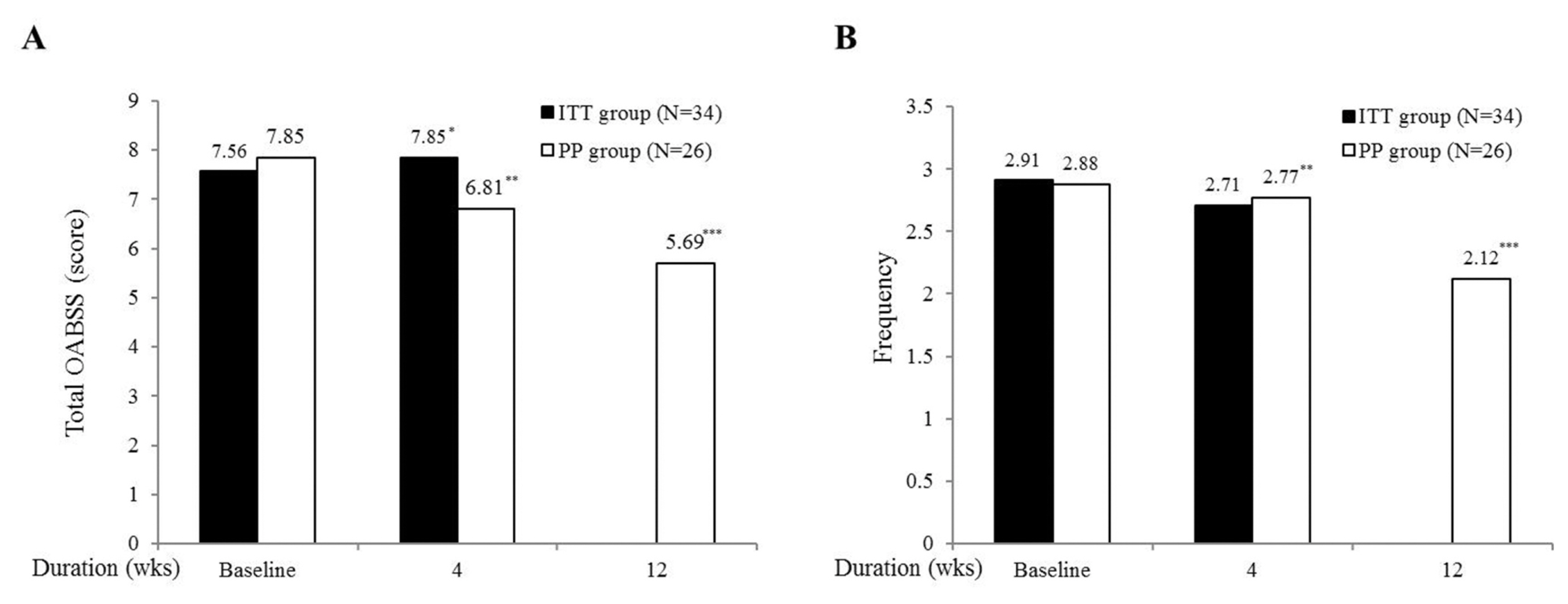
- From baseline to follow-up, mean total OABSS scores reduced in the PP group from 7.85 ± 3.08 (baseline) to 5.69 ± 3.08 (12 weeks, P < 0.001) (Fig. 2A). The PP group also showed the reduction of nocturia frequency from 2.88 ± 0.33 (baseline) to 2.12 ± 0.27 (12 weeks, P < 0.001) (Fig. 2B).
- Secondary efficacy outcome variables
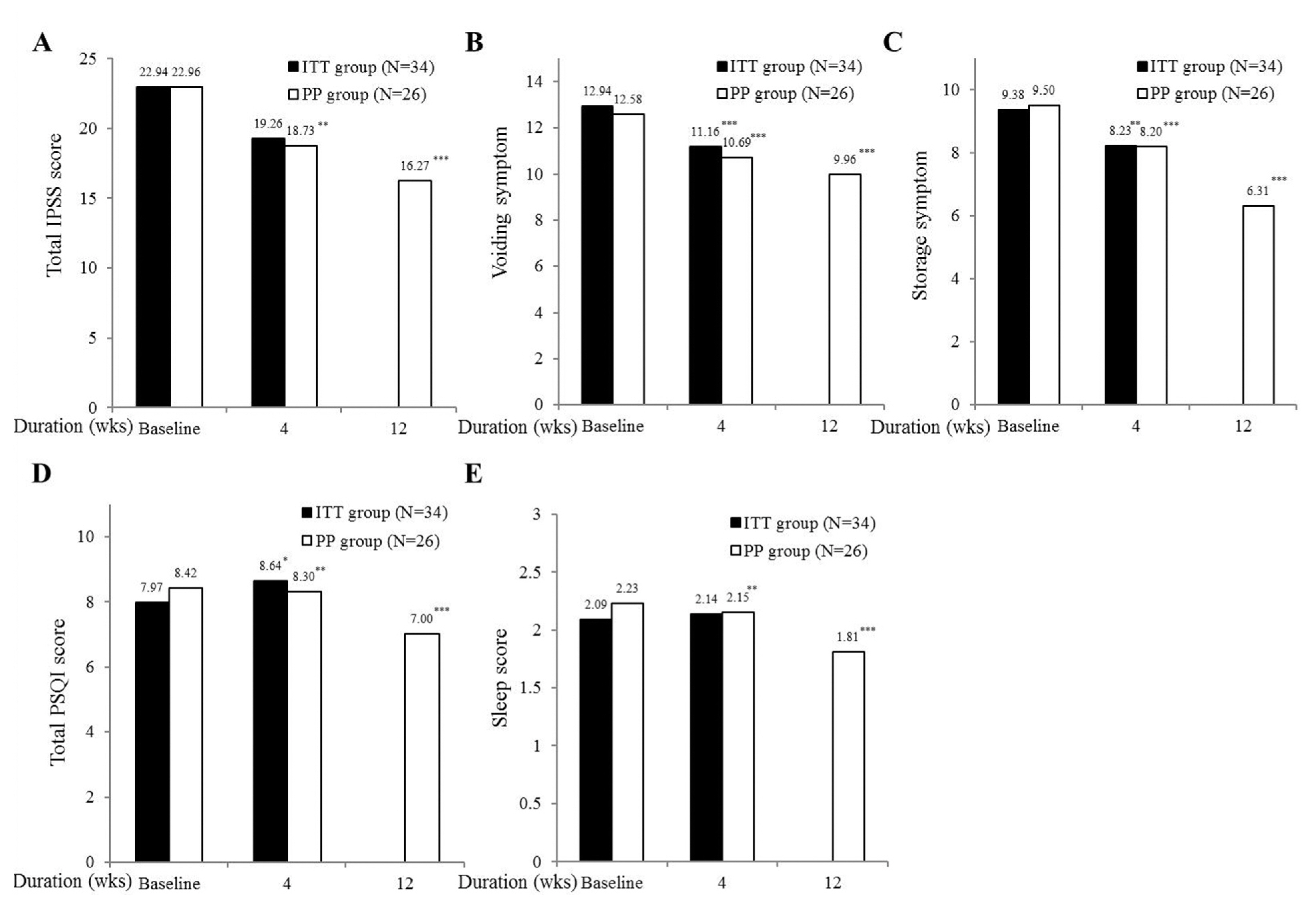
- Secondary endpoints were evaluated the change of total IPSS, voiding, and storage symptom in the PP group. From baseline to follow-up, mean total IPSS scores were reduced from 22.96 ± 7.92 (baseline) to 18.73 ± 5.23 (4 weeks, P < 0.01), 16.27 ± 5.39 (12 weeks, P < 0.001) (Fig. 3A). Overall voiding symptom scores was decreased from 12.58 ± 4.67 (baseline) to 10.69 ± 4.22 (4 weeks, P < 0.001), and 9.96 ± 4.12 (12 weeks, P < 0.001) (Fig. 3B). Storage symptom were also reduced from 9.5 ± 3.09 (baseline) to 8.2 ± 2.63 (4 weeks, P < 0.001), 6.31 ± 2.56 (12 weeks, P < 0.001) (Fig. 3C).
- Study participants were evaluated by using total PSQI and sleep quality to evaluate of the melatonin administration in the PP group. From baseline to follow-up, mean total PSQI scores were reduced from 8.42 ± 4.70 (baseline) to 7.0 ± 4.03 (12 weeks, P < 0.001) (Fig. 3D). Poor sleep quality were also reduced from 2.23 ± 0.59 (baseline) to 1.81 ± 0.57 (12 weeks, P < 0.001) (Fig. 3E).
- PP analysis including only patients with treatment compliance also showed improvement of WHO 5 quality of life scores from 10.15 ± 6.44 (baseline) to 13.54 ± 5.24 (12 weeks, P < 0.001) (Fig. 4).
- Safety and tolerability
- In total, 34 subjects who took at least one dose were included in the safety analysis of Circadin®. Patients with medication were generally well tolerated with no adverse event (AE) during the study or follow-up period. Adverse event was observed only one case (3.8%) with mild degree eyelid edema. This event was recovered spontaneously within 1 week. No clinically significant changes in laboratory tests, electrocardiogram, or blood pressure were observed in treatment group.
RESULTS
- In elderly, age-related changes in sleep depth and continuity affect normal circadian rhythm, and the normal circadian pattern of micturition as well. It is well known that the prevalence of nocturia increases with age which is associated with poor quality of life as well as self-reported insomnia.12 Nocturia is the most common bladder storage symptom in the general population.13 Three-quarters of participants in a survey of 8937 non-institutionalized individuals aged 18 years or over living in Texas, New York and California states residents of US cited the need to go to the bathroom as the most frequent reason for nocturnal awakenings. Indeed, going to the toilet was the primary reason for night-time awakening across all age groups, and the proportion affected increased with age: 39.9% in those aged 18–44 years to 77.1% in those aged 65 or above.5 Therefore, primary sleep hygiene tip is to improve sleep and nocturnal urinary frequency together in patients with LUTS/OAB.
- Nocturnal voids are regulated by circadian biological rhythms that include decreased nocturnal urine production through urine concentration via water reabsorption or through sodium retention, plasma renin angiotensin-aldosterone system, vasopressin with a peak diurnal rhythm during the night time hours, and atrial natriuretic peptide with important role in sodium excretion at night.14,15
- Currently, noctuira is treated successfully with various options including alpha blocker for prostate diseases, anticholinergics for bladder storage function and desmopressin for replacing antidiuretic hormone.16–18 Nevertheless, hypnotics and desmopressin increase the potential risk of dependency and hyponatremia, especially in the elderly. Therefore the new option to control nocturnal frequency and insomnia together is still required in the clinical field.
- Melatonin is a pineal gland hormone to exhibit a circadian rhythm, which shows low level during on daytime due to inhibition of its production by light and high level during night after onset darkness. Generally, it is considered melatonin is able to stabilize circadian rhythms, to reinforce them, and to maintain their phase-relationships, and thus, melatonin acts as an endogenous synchronizer of circadian rhythms and sleep is normally initiated when blood melatonin levels increase.19,20
- Melatonin has been found to have several physiologic effects on bladders in animal models, which include pelvic smooth muscle and bladder detrusor muscle tone adjustments (due to decreasing sympathetic tone), vascular tone adjustment, anti-oxidative effects (due to free radical scavenging), and anti-inflammatory effects, and to improve sleep quality.21–28 Matsuta et al. reported that exogenous melatonin increases bladder capacity vias γ-aminobutyric acidA receptor in the GABAergic system.29 These observations suggest melatonin could be beneficial for treating nocturia due to its effects on the central nervous system. Obayashi et al reported melatonin secretion was significantly and inversely associated with nocturia in a cohort study of an elderly population.30 This study was the first clinical study to evaluate the improvement of urination functions such as nocturia based on the anticholinergic action of melatonin on the bladder that was confirmed in animal experiments. These physiologic actions of melatonin are expected to enable normal voiding volumes and urinary frequencies by increasing functional bladder capacity, inter-contraction intervals, and threshold pressure and decreasing basal pressure on bladder (Fig. 5).
- We hypothesized that a reduction in symptoms of overactive bladder symptoms and improved sleep quality might be directly or indirectly achieved by administering melatonin, melatonin plus an alpha blocker, an anticholinergic agent, or an antidiuretic hormone. Circadin® (Kuhnil Pharm, Seoul, Korea) releases melatonin over 8–10 hours, and thus, should provide full night coverage, whereas nutritional supplements release it over 2–3 hours.6 The present clinical trial is meaningful because no previously study has investigated the role of melatonin on human bladder function from a clinical perspective. Our results show that 2 mg of prolonged release melatonin daily significantly improved almost all measures and was well tolerated with no adverse events leading to discontinuation. The reasons for drop-out of some study subjects (23.5%) were withdrawal of consent, non-compliance, and inclusion and exclusion violations during screening or the first 4 weeks of the clinical trial. This pilot study was performed as a global first clinical trial to investigate the effects of melatonin on bladder function. Although the findings of this study suggest that prolonged release melatonin has acceptable efficacy and safety, some limitations should be noted. First, the study design was established as non-placebo controlled, open label, single center study. Second, the present study was designed to have a relatively short period of treatment of 12 weeks. Long-term data are therefore needed as in other clinical trial studies. Third, the efficacy was not assessed according to the severity of chronic insomnia and overactive bladder. And comparison data was not shown with other treatment options. Future studies of prolonged release melatonin should include patients not to response to treatment such as failed those with current therapeutic modalities.
- These results was shown clearly that the clinical use of prolonged-release melatonin (Circadin®) in elderly patients with overactive bladder and chronic insomnia has the potential to control simultaneously voiding symptom and poor sleep quality even though it was not a placebo controlled long-term study. Based on these results, we suggest that prolonged release melatonin is sleep health enhancer with anti-cholinergic effect which can be used as primary prescription in patients with LUTS/OAB and sleep disorder together. Additionally sleep pattern should be evaluated on primary care of patients with urological disorders with BPH, LUTS or OAB.
DISCUSSION
Acknowledgments
ACKNOWLEDGEMENTS
-
CONFLICT OF INTEREST
The authors reported no conflicts of interest to declare in this article.
Article information
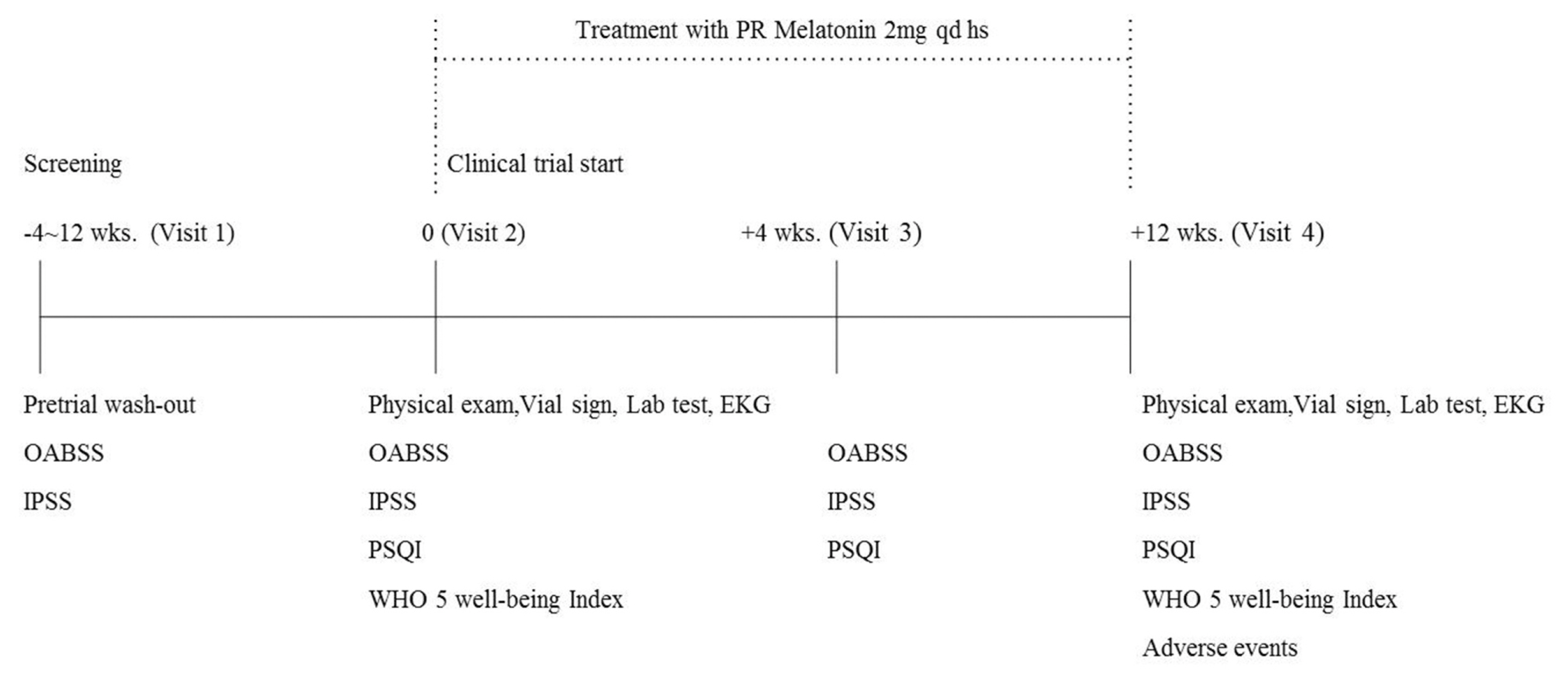
Fig. 2
Changes of total score of overactive bladder symptom score (OABSS) and nocturia frequency
(A) Total OABSS, (B) The nocturia frequency, Values are presented as mean ± standard deviation. *P > 0.05 vs baseline, ** P < 0.01 vs baseline, *** P < 0.001 vs baseline
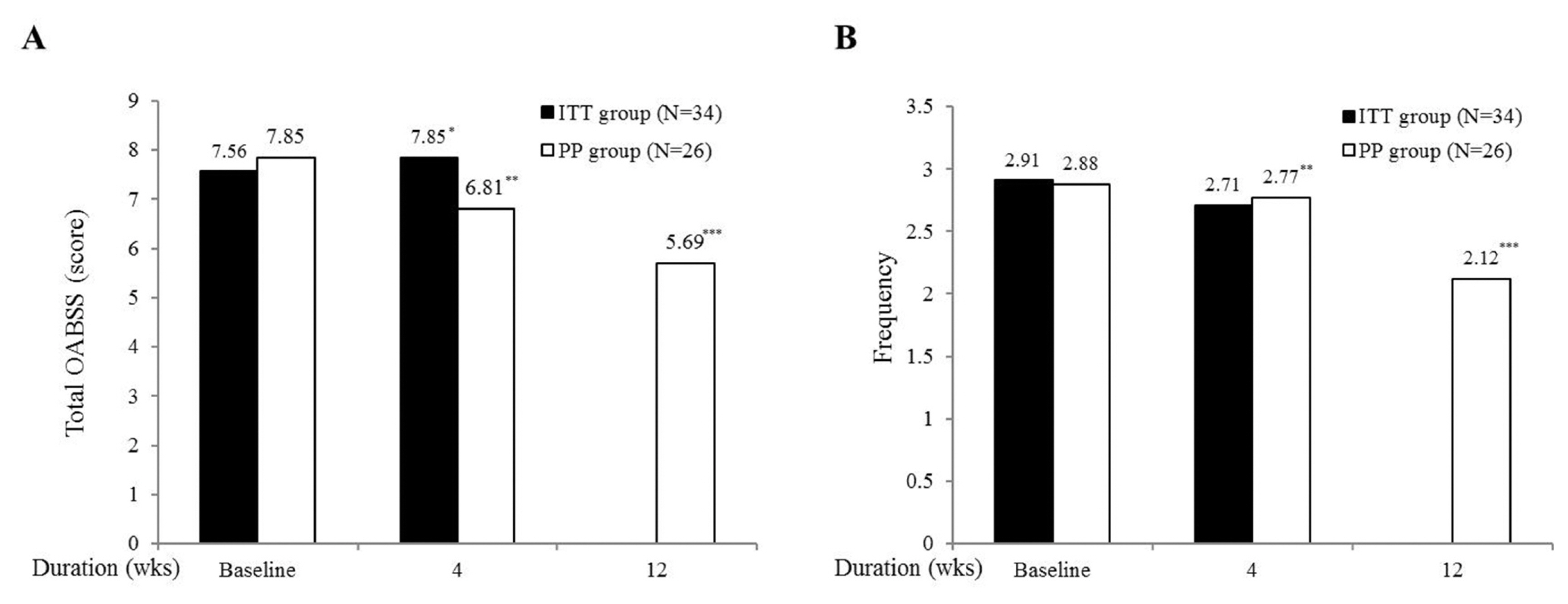
Fig. 3
Change in mean total IPSS, voiding and storage symptom, total PSQI, and sleep quality
(A) Total IPSS Score, (B) Voiding Symptoms, (C) Storage Symptoms, (D) Total PSQI Score, (E) Quality of Sleep * P > 0.05 vs baseline, ** P < 0.01 vs baseline, *** P < 0.001 vs baseline. Values are presented as mean ± standard deviation.
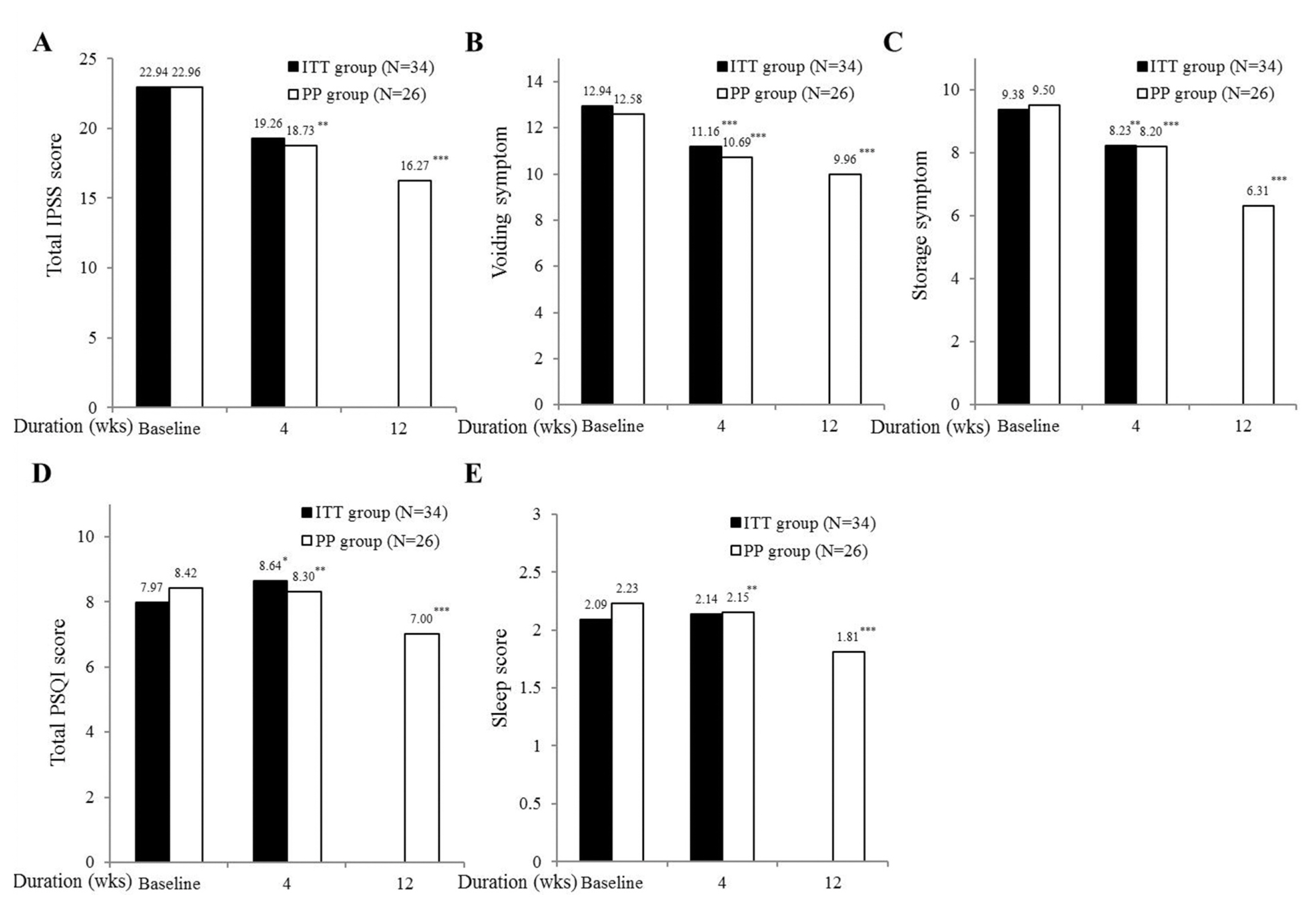
Fig. 4
Changes of quality of life by WHO 5 well-being index
Values are presented as mean ± standard deviation.* P < 0.001 vs baseline

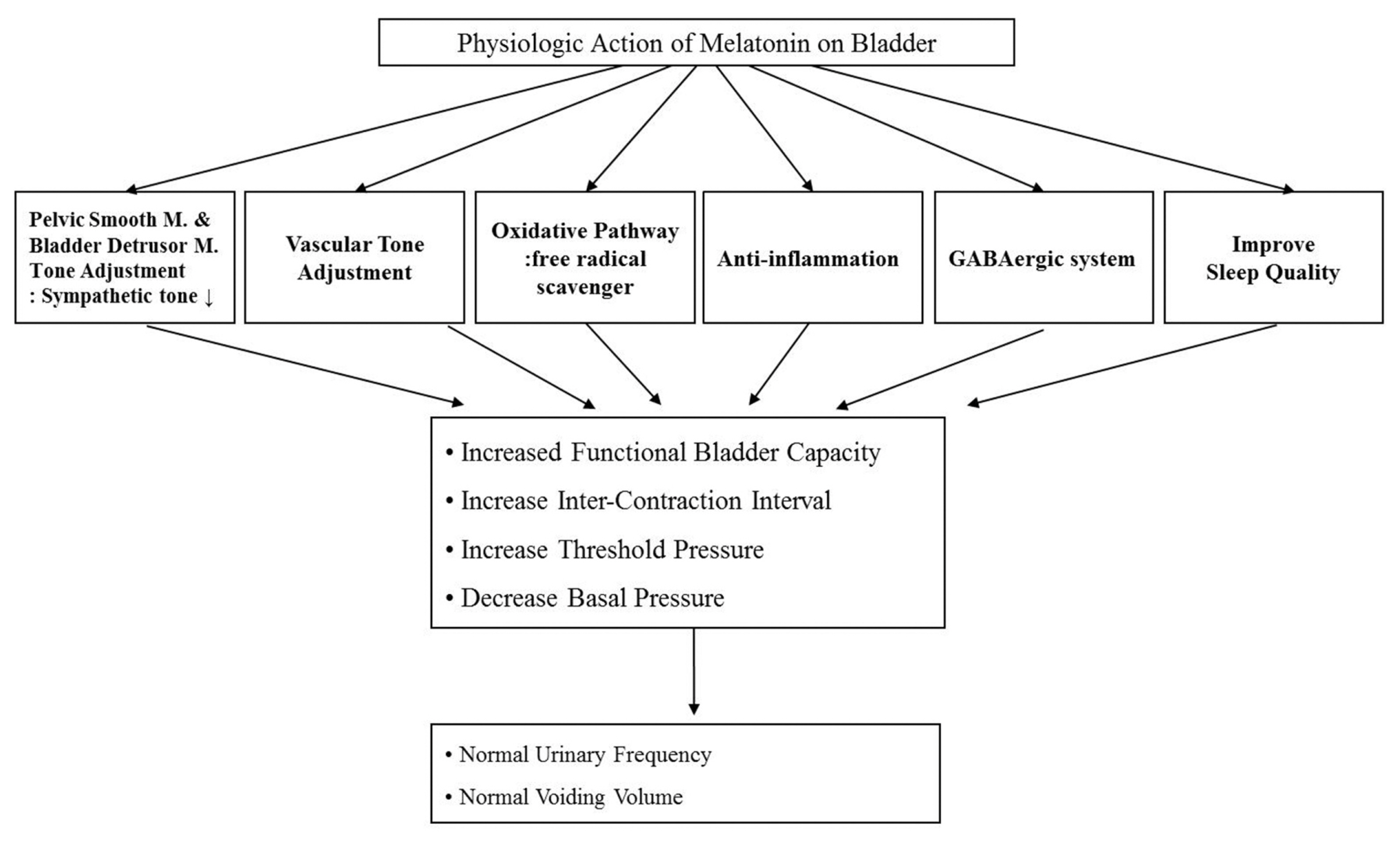
Table 1Clinical profile of patients
- 1. Kryger MH, Roth T, Dement WC. Principles and practice of sleep medicine. 5th ed. Philadelphia (PA): Elsevier Saunders; 2010. p. p489–90.
- 2. Chartier-Kastler E, Leger D, Comet D, Haab F, Ohayon MM. Prostatic hyperplasia is highly associated with nocturia and excessive sleepiness: a cross-sectional study. BMJ Open 2012;30:e000505.Article
- 3. Kim SC, Kim SW, Chung YJ. Men’s health in South Korea. Asian J Androl 2011;13:519–25.ArticlePubMedPMC
- 4. Cho JW, Duffy JF. Sleep, Sleep Disorders, and Sexual Dysfunction. World J Mens Health 2019;37:261–75.ArticlePubMed
- 5. Ohayon MM. Nocturnal awakenings and comorbid disorders in the American general population. J Psychiatr Res 2008;43:48–54.ArticlePubMed
- 6. Aldhous M, Franey C, Wright J, Arendt J. Plasma concentrations of melatonin in man following oral absorption of different preparations. Br J Clin Pharmacol 1985;19:517–21.ArticlePubMedPMC
- 7. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28:193–213.ArticlePubMed
- 8. Jeong SJ, Homma Y, Oh SJ, Jeong SJ. Korean version of the overactive bladder symptom score questionnaire: translation and linguistic validation. Int Neurourol J 2011;15:135–42.ArticlePubMedPMC
- 9. Kim JH, Doo SW, Yang WJ, Song YS. Homogeneity among the korean international prostate symptom score questionnaires used in real practice. Korean J Urol 2013;54:249–51.ArticlePubMedPMC
- 10. Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med Rev 2016;25:52–73.ArticlePubMed
- 11. Moon YS, Kim HJ, Kim DH. The relationship of the Korean version of the WHO Five Well-Being Index with depressive symptoms and quality of life in the community-dwelling elderly. Asian J Psychiatr 2014;9:26–30.ArticlePubMed
- 12. Griebling TL. Incidence and Remission of Nocturia: A Systematic Review and Meta-Analysis. J Urol 2016;196:1710–1.PubMed
- 13. Irwin DE, Milsom I, Kopp Z, Abrams P, Artibani W, Herschorn S. Prevalence, severity, and symptom bother of lower urinary tract symptoms among men in the EPIC study: impact of overactive bladder. Eur Urol 2009;56:14–20.ArticlePubMed
- 14. Thomas S. Some effects of changes of posture on water and electrolyte excretion by the human kidney. J Physiol 1957;139:337–52.PubMedPMC
- 15. George CP, Messerli FH, Genest J, Nowaczynski W, Boucher R, Kuchel Orofo-Oftega M. Diurnal variation of plasma vasopressin in man. J Clin Endocrinol Metab 1975;41:332–8.ArticlePubMed
- 16. Ohashi M, Fujio N, Nawata H, Kato K, Ibayashi H, Kangawa K, et al. High plasma concentrations of human atrial natriuretic polypeptide in aged men. J Clin Endocrinol Metab 1987;64:81–5.ArticlePubMed
- 17. Roehrborn CG, Van Kerrebroeck P, Nordling J. Safety and efficacy of alfuzosin 10 mg once-daily in the treatment of lower urinary tract symptoms and clinical benign prostatic hyperplasia: a pooled analysis of three double-blind, placebo-controlled studies. BJU Int 2003;92:257–61.ArticlePubMed
- 18. Choi S, Cho WY, Min K, Lee JZ, Moon KH, Kwon T, et al. Influence of daytime or nighttime dosing with solifenacin for overactive bladder with nocturia: impact on nocturia and sleep quality. J Korean Med Sci 2017;32:1491–5.ArticlePubMedPMC
- 19. Weiss JP, Wein AJ, van Kerrebroeck P, Dmochowski R, Fitzgerald M, Tikkinen KA, et al. Nocturia: new directions. Neurourol Urodyn 2011;30:700–3.ArticlePubMed
- 20. Claustrat B, Brun J, Chazot G. The basic physiology and pathophysiology of melatonin. Sleep Med Rev 2005;9:11–24.ArticlePubMed
- 21. Zisapel N. New perspectives on the role of melatonin in human sleep, circadian rhythms and their regulation. Br J Pharmacol 2018;175:3190–9.ArticlePubMedPMC
- 22. Fathollahi A, Daneshgari F, Hanna-Mitchell AT. Melatonin and its role in lower urinary tract function: An article review. Curr Urol 2015;8:113–8.ArticlePubMedPMC
- 23. Gomez-Pinilla PJ, Gomez MF, Swärd K, Hedlund P, Hellstrand P, Camello PJ, et al. Melatonin restores impaired contractility in aged guinea pig urinary bladder. J Pineal Res 2008;44:416–25.ArticlePubMed
- 24. Han JH, Chang IH, Myung SC, Lee MY, Kim WY, Lee SY, et al. A novel pathway underlying the inhibitory effects of melatonin on isolated rat urinary bladder contraction. Korean J Physiol Pharmacol 2012;16:37–42.ArticlePubMedPMC
- 25. Dobrek Ł, Thor PJ. The influence of melatonin and agomelatine on urodynamic parameters in experimental overactive bladder model-preliminary results. Postepy Hig Med Dosw (Online) 2011;65:725–33.ArticlePubMed
- 26. Semerciöz A, Onur R, Ayar A, Orhan I. The inhibitory role of melatonin on isolated guinea-pig urinary bladder: an endogenous hormone effect. BJU Int 2004;94:1373–6.ArticlePubMed
- 27. Juszczak K, Ziomber A, Machowska A, Furgała A, Dobrek Ł, Wyczółkowski M, et al. The ameliorating effect of exogenous melatonin on urinary bladder function in hyperosmolar bladder overactivity and its influence on the autonomic nervous system activity. Acta Medica (Hradec Kralove) 2011;54:63–8.ArticlePubMed
- 28. Sener G, Sehirli AO, Paskaloğlu K, Dülger GA, Alican I. Melatonin treatment protects against ischemia/reperfusion-induced functional and biochemical changes in rat urinary bladder. J Pineal Res 2003;34:226–30.ArticlePubMed
- 29. Sener G, Atasoy BM, Ersoy Y, Arbak S, Sengöz M, Yeğen BC. Melatonin protects against ionizing radiation-induced oxidative damage in corpus cavernosum and urinary bladder in rats. J Pineal Res 2004;37:241–6.ArticlePubMed
- 30. Matsuta Y, Yusup A, Tanase K, Ishida H, Akino H, Yokoyama O. Melatonin increases bladder capacity via GABAergic system and decreases urine volume in rats. J Urol 2010;184:386–91.ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Melatonin and melatonin receptor agonists in the treatment of nocturia: A systematic review
Christine Anh Burke, Victor W. Nitti, Lynn Stothers
Neurourology and Urodynamics.2024; 43(4): 826. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite