KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 35(1); 2020 > Article
-
Case Reports
Klebsiella pneumoniae -induced Liver Abscess Complicated with Septic Pulmonary Embolism in a Non-diabetic Adult - Byung Hun Lim, Song-I Lee
-
Kosin Medical Journal 2020;35(1):69-75.
DOI: https://doi.org/10.7180/kmj.2020.35.1.69
Published online: June 30, 2020
1Department of Internal Medicine, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea
2Department of Internal Medicine, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea
- Corresponding Author: Song-I Lee, Department of Internal Medicine, College of Medicine, Chungnam National University, 282, Munhwa-ro, Jung-gu, Daejeon 35015, Korea, Tel: +82-42-280-7870, E-mail: newcomet01@naver.com
• Received: March 2, 2020 • Revised: April 14, 2020 • Accepted: May 6, 2020
Copyright © 2020 by Korean Association of Medical Journal Editors
Articles published in Kosin Medical Journal are open-access, distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,253 Views
- 7 Download
Abstract
- A 72-year-old non-diabetic man was admitted to the intensive care unit because of liver abscess, cholecystitis, and septic shock. He underwent percutaneous catheter drainage and received intravenous antibiotics. Shock was improved, and the patient’s fever subsided. Klebsiella pneumoniae was isolated in blood and bile cultures. However, he suddenly developed dyspnea and oxygen desaturation. Chest computed tomography scan revealed multifocal ground-glass opacities with consolidation with peripheral preponderance. Appropriate antibiotic therapy was provided for 2 weeks. The patient recovered fully, and cholecystectomy was then performed. Herein, we report a case of K. pneumoniae-induced liver abscess complicated with septic pulmonary embolism in a non-diabetic patient.
- A previously healthy 72-year-old man visited the emergency room because of fever and right upper abdominal pain. He had been diagnosed with hypertension 10 years previously and was on medication for hypertension. He had nonspecific family history and had stopped smoking 5 years ago (50 pack-years).
- Physical findings were as follows: blood pressure, 117/61 mmHg; pulse rate, 92 beats/minute; respiratory rate, 21 cycles/minute; and body temperature, 38.7°C. Moreover, the patient was alert, and his breathing sounds were normal. On the basis of an abdominal examination, the patient had right upper abdominal tenderness, and Murphy sign was observed.
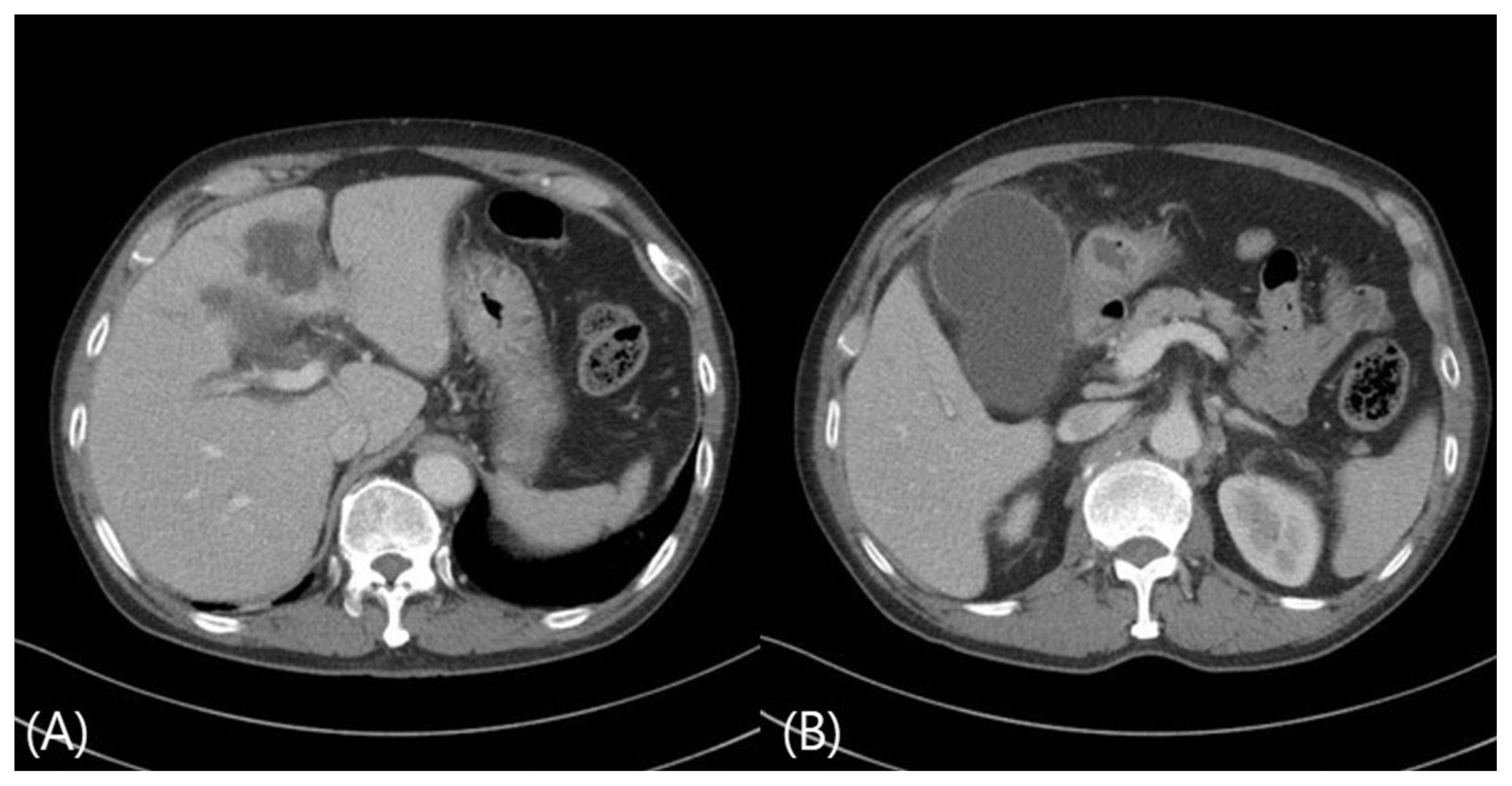
- The peripheral blood test results were as follows: white blood cell count, 9,900 mm3 (neutrophil: 98.0%, lymphocyte: 1.8%, and monocytes: 0.2%). hemoglobin level, 11.3 mg/dL; platelet count, 128,000/mm3. Meanwhile, serum biochemistry was performed, and the results were as follows: aspartate aminotransferase level,156 IU/L; and alanine aminotransferase level, 156/58 IU/L, alkaline phosphatase level, 174 U/L; γ-glutamyl transpeptidase level, 280 IU/L; total bilirubin level, 2.10 mg/dL; lactate dehydrogenase level, 872 U/L; blood glucose level, 87 mg/day; glycated hemoglobin (HbA1c) level, 6.0%; and C-reactive protein level, 17.4 mg/dL. The patient tested negative for hepatitis B surface antigen and anti-hepatitis C Ab and positive for anti-HB antibody. K. pneumoniae was detected in two pairs of blood culture and one pair of bile culture. Simple chest radiography and chest CT scan were performed at the emergency room, and no specific findings were obtained, except for emphysema and bronchitis (Fig. 1). Moreover, abdominal CT scan revealed the presence of a liver abscess in segment 4 (4.5 cm × 3.7 cm) and a dilated gallbladder with diffuse inflammatory thickening (Fig. 2).
- The blood pressure of the patient immediately dropped to 80/40 mmHg after the emergency room visit. However, it normalized after hydration and administration of vasopressor. Percutaneous drainage was performed for cholecystitis, and the patient was admitted in the intensive care unit (ICU) due to liver abscess. Treatment with ciprofloxacin and metronidazole was initiated. On the second day of hospitalization, the patient’s blood pressure remained within normal range even without the use of a vasopressor. Thus, he was transferred to the general ward.
- However, on the fourth day, the patient presented with difficulty breathing and fever, which subsequently worsened. The patient’s oxygen saturation decreased to 89% even with high-flow oxygen therapy (fraction of inspired oxygen [FiO2]: 80%, flow: 50 L). Multiple chest GGO and consolidation were observed on chest CT scan. The patient was again admitted to the ICU because of suspected nonspecific pneumonia. On the fourth day, K. pneumoniae was identified in the blood culture, and antibiotic susceptibility tests revealed susceptibility to all antibiotics, except ampicillin. However, as the patient’s condition worsened and fever persisted, the antibiotics were changed to piperacillin/tazobactam and metronidazole.
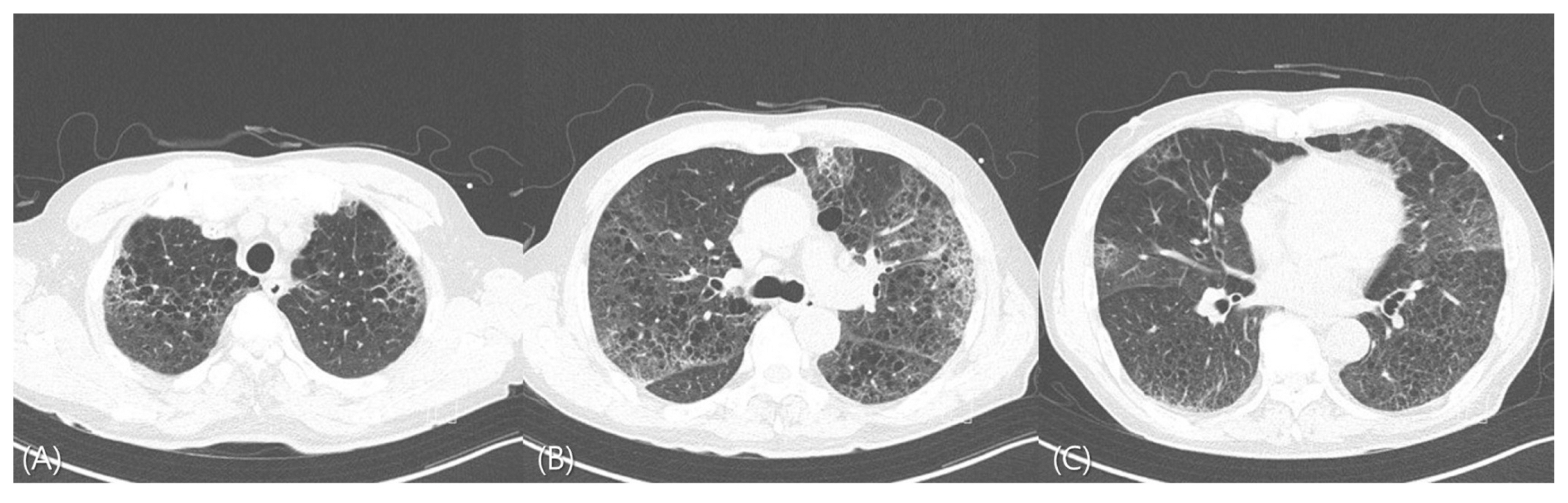
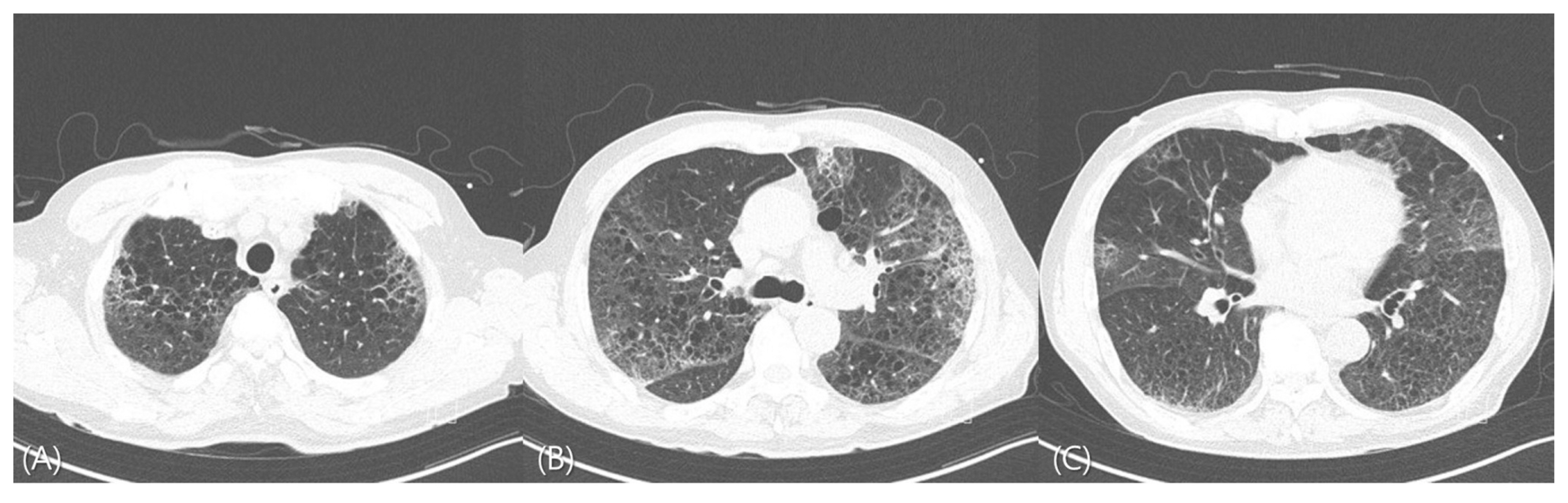
- On the sixth day of hospitalization, the patient did not present with fever, and K. pneumoniae was identified in one pair of bile culture. On the seventh day, his oxygen demand decreased (FiO2: 50%, flow: 35 L). Chest CT scan was then performed, and results revealed bilateral multiple GGO and consolidation (Fig. 3). The patient’s C-reactive protein level decreased to 5.9 mg/dL. The presence of bacteria was not identified in the blood culture performed on the fifth day and thereafter.
- The patient did not complain of conjunctival bleeding or decreased visual acuity. However, he was referred to an ophthalmologist for the examination for endophthalmitis caused by K. pneumoniae. Other than cataracts, no specific findings were observed. After the administration of piperacillin/tazobactam and metronidazole, all clinical symptoms improved. The patient was prescribed oral moxifloxacin as home medication and was then discharged. Since then, the patient has undergone a cholecystectomy in the department of surgery. The patient is currently being followed up in the outpatient department.
CASE
- Pyogenic liver abscess is a common infection that occurs in the abdominal cavity and is often transmitted directly from biliary tract infections and, sometimes, bacteremia. However, the other causes are unknown.2 E. coli was found to be a common causative organism in Korea before the 1980s; since then, the organism has been considered a common causative agent.1 K. pneumoniae was identified as an emerging cause of community-acquired liver abscess in Korea.8
- K. pneumoniae liver abscess is frequently associated with septic metastatic lesions, endogenous endophthalmitis, cerebral abscess, meningitis, and infectious spondylitis.9–12 An invasive K. pneumoniae liver abscess syndrome is defined as K. pneumoniae-induced liver abscess that is accompanied by metastatic infections involving an organ other than the liver.2 Among these infections, septic pulmonary embolism is not common, and the diagnosis is often delayed. In a study conducted in Taiwan, the common symptoms of septic pulmonary embolism associated with K. pneumoniae liver abscess were fever and dyspnea, and chest CT scan revealed nodules, pleural effusions, and wedge-shaped lesions involving the margins of the lungs, with or without the cavities.4 In this patient, K. pneumoniae was not identified in sputum culture, but in other studies, K. pneumoniae was confirmed in sputum in only 3 out of 9 patients with septic embolism accompanying K. pneumonia liver abscess.13 And another study showed negative findings in sputum culture (n = 9) and endobronchial culture (n = 5) among 14 patients.4 Thus, the sensitivity of sputum culture is found to be around 50%,14 so the imaging work up is more emphasized in pulmonary septic embolism.
- Diabetes is a risk factor for K. pneumoniae-induced liver abscess, and about 80% of patients with diabetes due to an underlying disease present with K. pneumoniae liver abscess.15 Patients with uncontrolled blood sugar levels are at higher risk of gas-forming liver abscesses, liver abscesses of unknown origin, and metastatic infections than those with controlled blood sugar levels. Liver abscesses of unknown origin and metastatic infections are more common in groups with poor blood sugar control (HbA1c > 10%). HbA1c levels and abscess size < 5 cm are independent risk factors for the metastatic complications of K. pneumoniae liver abscess.16 This patient was an ex-smoker and had an emphysematous change in the lungs, and it was thought that the appearance of K. pneumoniae bacteremia due to liver abscess with cholecystitis caused micro embolism, resulting in septic pulmonary embolism.
- Septic pulmonary embolism can be identified based on the presence of a nodule in the parenchyma, including the pulmonary margins and various cavities and blood vessels supplying them, and heterogeneous, wedge-shaped lesions in the pleura.4,13 However, the differential diagnoses of several pulmonary nodules include tuberculosis, fungal infections, and tumors. The disappearance of pulmonary nodules after proper antimicrobial therapy is an indication that the diagnosis of septic pulmonary embolism is correct. However, other examinations should also be performed to rule out other potential causes of pulmonary lesions.
- In this case, the non-diabetic patient was diagnosed with liver abscess associated with cholecystitis. K. pneumoniae was identified in the blood and bile cultures. Based on the initial chest radiography, there were no specific findings, except for emphysema and bronchitis. However, in the general ward, the patient presented with hypoxemia and dyspnea while on antibiotic treatment. Thus, chest CT scan was performed and revealed multiple GGO with consolidation. The patient was treated in the ICU because of suspected metastatic lung infection. The sputum cultures did not reveal the presence of K. pneumoniae probably because the test was performed after antibiotic treatment and the probability of culturing was low.
- The mortality rate of septic pulmonary embolism associated with liver abscess is as high as 14%.4 Therefore, when patients with K. pneumoniae liver abscess complain of fever and respiratory symptoms, the possibility of septic pulmonary embolism should be considered. Thus, active evaluation, such as performing imaging and sputum tests, must be performed, and treatment should be provided.
DISCUSSION

Fig. 2Abdominal computed tomography scan revealed a 4.5-cm liver abscess in segment 4 of the liver (A) and a dilatated gallbladder with diffuse inflammatory thickening (B).

Fig. 3Chest computed tomography scan revealed multifocal ground-glass opacities with consolidation in both upper lung fields (A), the right middle lung (B), and the lingular segment of the left upper lung with peripheral preponderance (C).
- 1. Chung DR, Lee SS, Lee HR, Kim HB, Choi HJ, Eom JS, et al. Emerging invasive liver abscess caused by K1 serotype Klebsiella pneumoniae in Korea. J Infect 2007;54:578–83.ArticlePubMed
- 2. Siu LK, Yeh KM, Lin JC, Fung CP, Chang FY. Klebsiella pneumoniae liver abscess: a new invasive syndrome. Lancet Infect Dis 2012;12:881–7.ArticlePubMed
- 3. Lim SW, Lee EJ, Lee SW, Kim SM, Kim JH, Kim BJ, et al. Clinical significance of Klebsiella pneumoniae in liver abscess. Korean J Gastroenterol 2003;42:226–31.PubMed
- 4. Chou DW, Wu SL, Chung KM, Han SC. Septic pulmonary embolism caused by a Klebsiella pneumoniae liver abscess: clinical characteristics, imaging findings, and clinical courses. Clinics (Sao Paulo) 2015;70:400–7.ArticlePubMedPMC
- 5. Lee SJ, Cha SI, Kim CH, Park JY, Jung TH, Jeon KN, et al. Septic pulmonary embolism in Korea: Microbiology, clinicoradiologic features, and treatment outcome. J Infect 2007;54:230–4.ArticlePubMed
- 6. Kamano Y, Ohashi H, Kikuchi T, Watanabe K, Kitahara M. Liver abscess and Aeromonas bacteremia with septic pulmonary embolism. Intern Med 2003;42:1047–9.ArticlePubMed
- 7. Ryung YJ, Yeop Y, Na JY, Sook LH, Ho JG, Ina J. Klebsiella pneumoniae Liver abscess complicated with septic pulmonary embolism. J Korean Geriatr Soc 2013;17:239–43.Article
- 8. Chung DR, Lee SS, Lee HR, Kim HB, Choi HJ, Eom JS, et al. Emerging invasive liver abscess caused by K1 serotype Klebsiella pneumoniae in Korea. J Infect 2007;54:578–83.ArticlePubMed
- 9. Lee KH, Moon SY, Kim IA, Kwon SY, Kim JH, Choe WH, et al. A Case of Delayedonset Multiple Metastatic Infection following Liver Abscess. Korean J Gastroenterol 2015;66:237–41.PubMed
- 10. Kim GS, Lee JH, Choi SA, Lim SR. A case of Klebsiella pneumoniae liver abscess complicated with brain abscess and endophthalmitis. J Korean Neurol Assoc 2005;23(5):78–80.
- 11. Yoon HS, Lee MH, Lee SJ, Kim KY, You YP, Jung DY, et al. A Case of pyogenic liver abscess complicated with endophthalmitis. Korean J Gastroenterol 2001;38:120–3.
- 12. Chiu CT, Lin DY, Liaw YF. Metastatic septic endophthalmitis in pyogenic liver abscess. J Clin Gastroenterol 1988;10:524–7.ArticlePubMed
- 13. Yang PW, Lin HD, Wang LM. Pyogenic liver abscess associated with septic pulmonary embolism. J Chin Med Assoc 2008;71:442–7.ArticlePubMed
- 14. Marrie TJ, Poulin-Costello M, Beecroft MD, Herman-Gnjidic Z. Etiology of community-acquired pneumonia treated in an ambulatory setting. Respir Med 2005;99:60–5.ArticlePubMed
- 15. Fung CP, Chang FY, Lee SC, Hu BS, Kuo BI, Liu CY, et al. A global emerging disease of Klebsiella pneumoniae liver abscess: is serotype K1 an important factor for complicated endophthalmitis? Gut 2002;50:420–4.ArticlePubMedPMC
- 16. Lin YT, Wang FD, Wu PF, Fung CP. Klebsiella pneumoniae liver abscess in diabetic patients: association of glycemic control with the clinical characteristics. BMC Infect Dis 2013;13:56.ArticlePubMedPMC
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite