KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 35(1); 2020 > Article
-
Original Articles
Clinical Usefulness of Contrast-Enhanced Computed Tomography in Patients with Non-Obstructive Acute Pyleonephritis - In O Sun, Ji Hye Lim, Ju Hwan Oh, A Young Cho, Beum Jin Kim, Kwang Young Lee, Mi Sook Lee
-
Kosin Medical Journal 2020;35(1):38-46.
DOI: https://doi.org/10.7180/kmj.2020.35.1.38
Published online: June 30, 2020
1Division of Nephrology, Department of Internal Medicine, Presbyterian Medical Center, Jeonju, Korea
2Department of Radiology, Presbyterian Medical Center, Jeonju, Korea
- Corresponding Author: Mi Sook Lee, Department of Internal Medicine, Presbyterian Medical Center, 365, Seowonro, Wansan-Gu, Jeonju 54987, Korea, Tel: +82-63-230-1332, Fax: +82-63-230-1309, E-mail: ms0928l@nate.com
• Received: March 23, 2020 • Revised: April 13, 2020 • Accepted: May 6, 2020
Copyright © 2020 by Korean Association of Medical Journal Editors
Articles published in Kosin Medical Journal are open-access, distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,107 Views
- 2 Download
Abstract
-
Objectives
- The aim of this study is to investigate the clinical utility of contrast-enhanced computed tomography (CE-CT) in patient with non-obstrcutive acute pyelonephritis (APN).
-
Methods
- From 2007 to 2013, 537 APN patients who underwent a CE-CT scan within 24 hours after hospital admission were enrolled. We divided these patients into greater (50% or greater involvment, n = 143) and lesser (less than 50% involvement, n = 394) groups based on renal parenchymal involvement in CE-CT examination. We compared clinical characteristics between two groups and analyzed the clinical value of CE-CT scan as a reliable marker for predicting clinical severity and disease course in patient with non-obstructive APN.
-
Results
- The mean estimated glomerular filtration rate was 70.6 ± 25.5 mL/min/1.73m2. Compared with patients in lesser group, the patients in greater group had lower serum albumin levels (3.5 ± 0.5 vs 3.8 ± 0.6, P < 0.01) and longer hosptal stay (10.1 ± 4.7 vs 8.8 ± 4.5, P < 0.05). In addition, acute kidney injury (AKI) (23.1% vs 11.4%, P < 0.005) and bacteremia (36.4% vs 26.8%, P = 0.02) were frequently developed in greater group, respectively. The overall incidence of AKI was 14.8% based on RIFLE criteria. In a multivariate logistic regression analysis for predciting AKI, age, presence of diabetes mellitus and the presence of renal parenchymal involvement of greater than 50% in CE-CT were significant predictors of AKI.
-
Conclusions
- The CE-CT scan could be useful to predict the clinical severity and course in non-obstructive APN patients with preserved renal function.
- Patient selection
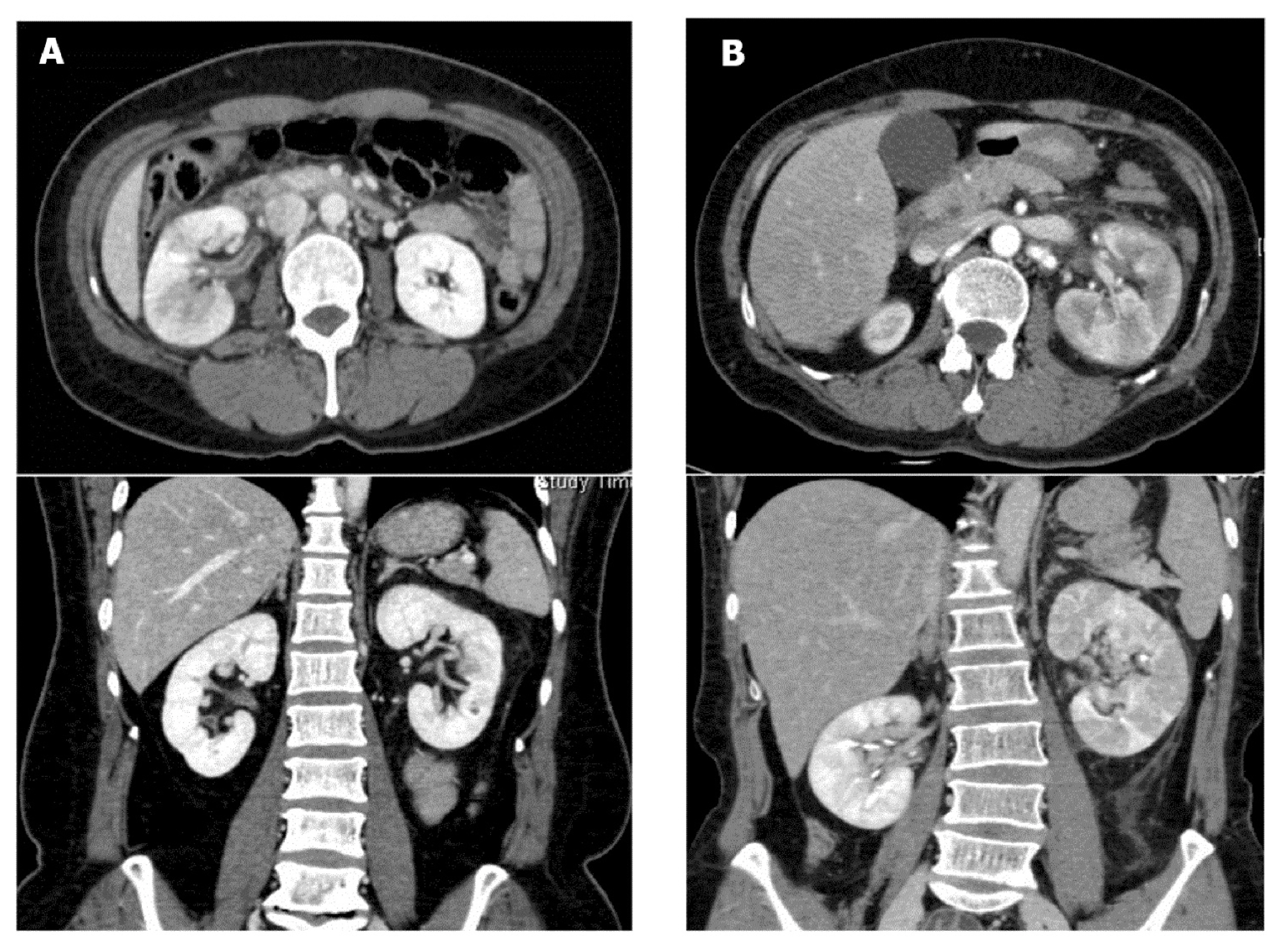
- From January 2007 to December 2013, we enrolled 556 APN patients who underwent a CE-CT scan within 24 hours after hospital admission before starting antibiotic treatment. Patients were excluded if they were younger than 18 years or had an hydronephrosis or renal abscess on CT scan. We also excluded the patients with post-contrast induced-acute kidney injury (CI-AKI) or low-quality image due to various causes. A clinical diagnosis of APN was made in patients with more than three of the following five diagnostic criteria: (1) clinical symptoms such as fever, chills, vomiting, or flank pain (2) costovertebral angle tenderness (3) fever of higher than 37.5 °C (4) leukocytosis in the complete blood count (5) abnormal urine test results (pyuria: white blood cell of ≥ 10/high-power field or positive urine culture of 105 colony-forming unit/mL). A total of 537 patients were included in this study. Two experienced radiologist divided these patients into two groups by approximately quantifying renal parenchymal low density extent on CE-CT. APN extent was approximately quantified on CE-CT by calculating number of slices that contained less enhancing lesion divided by total number of slices that contained normal renal parenchyma (Fig. 1). We also checked the status of renal parenchymal involvement. In cases with bilateral APN of different grades in each kidney, the higher grade was recorded. Patients were divded into two groups: greater group (greater than 50% involvement, n = 143) and lesser group (lesser than 50% involvement, n = 394). This study was approved by the Institutional Review Board of the Presbyterian Medical Center, Jeonju, South Korea (IRB No. 2019-05-014).
- Clinical and laboratory information
- All patients had a detailed clinical history and examination, a standard set of investigations including complete blood counts, liver function tests, serum creatinine, urea, electrolytes, chest radiograph, three peripheral blood smears for malaria, urinalysis, and two blood cultures. AKI was defined based on the RIFLE (Risk, Injury, Failure, Loss of kidney function, and End-stage kidney disease) criteria,9 and patients were categorized into the R, I or F categories. We defined CI-AKI with the RIFLE criteria as a relative increment in serum creatinine of ≥ 50%, or a decrease in estimated glomerular filtration rate of ≤ 25% from baseline, or an episode of oliguria lasting ≥ 6 hours within 48 to 72 hours following contrast administration.10 The estimated glomerular filtration rate (eGFR) was calculated using the abbreviated Modification of Diet in Renal Disease (MDRD) equation.11 When the baseline serum creatinine was not available, it was calculated using the standard four-variable MDRD formula assuming eGFR of 75 mL/min/1.73 m2. The RIFLE class was determined based on the worst among serum creatinine levels, eGFR, and urine output criteria. Renal replacement therapy was initiated using the standard indications. Sepsis is defined as the presence (probable or documented) of infection together with systemic manifestations of renal infection. The CT images were reviewed by two radiologists who unaware of clinical information; the final decision of grade was reached by consensus.
- CT technique
- CT scan was conducted on a 16-channel multi-detector row scanner (Somatom Sensation 16, Siemens Medical Solutions, Erlangen, Germany) with setting of 3 mm slice thickness. The CT findings were evaluated in the neprographic phases. Intravenous contrast material was administrated in an antecubital vein with injector at a dose of 1.5 mL/Kg body weight at a rate of 3 mL/s to a maximum of 120 mL. Nephrographic-phase scans were started 90 to 100 seconds after contrast injection.
- Statistical analysis
- All data are presented as means ± standard deviations unless otherwise specified. The baseline characteristics of patients in the greater and lesser groups were compared using t tests for continuous variables and chi-square tests for categorical variables. Clinically relevant parameters or the variables that were significantly associated with the presence of AKI in the univariate analysis were included in the multivariate analysis. A P-value of < 0.05 was considered to be statistically significant. All statistical analyses were carried out using SPSS version 22.0.
METRIALS AND METHODS
- Baseline characteristics
- The baseline characteristics of the 537 study subjects are presented in Table 1. The patients included 504 (93.9%) men and 33 (6.1%) women, with a mean age of 55.2 ± 17.9 years. The mean estimated glomerular filtration rate was 70.6 ± 25.5 mL/min/1.73m2. The initial white blood cell count (WBC) and serum albumin levels were 12.7 × 103/mL and 3.8 g/dL, respectively. The mean hospital stay was 9.2 ± 4.6 days. Bilateral renal involvement in CE-CT and bacteremia were noted in 18.2% and 29.4% of the patients, respectively. Of 537 participants, 78 (14.5%) experienced AKI during hospitalization period.
- Comparison of clinical characteristics between greater and lesser group
- When we compared clinical characteristics between greater (n = 143) and lesser (n = 394) groups, the patients in greater group had lower serum albumin levels (3.5 ± 0.5 vs 3.8 ± 0.6, P < 0.01) and longer hospital stay (10.1 ± 4.7 vs 8.8 ± 4.5, P < 0.05). Furthermore, bilateral renal involvement (40.6% vs 10.2%, P < 0.05) and bacteremia (36.4% vs 26.9%, P < 0.05) were frequently developed in greater group, respectively (Table 2). AKI (23.1% vs 11.4%, P < 0.05) occurred more frequently in greater group than lesser group. According to the RIFLE criteria, 52 (66.6%) and 26 (33.4%) in our study fell into the R and I categories, respectively. By univariate analysis, age, presence of diabetes mellitus or hypertension, serum albumin, total leukocyte count, bilateral renal involvement and 50% or greater renal parenchymal involvement in CT scan were significant predictors of AKI. Adjusting for these factors in a multivariate logistic regression analysis, older age and CT finding of 50% or greater renal parenchymal involvement were the only significant predictors of AKI (Table 3).
RESULTS
- In the present study, we show that the patients in greater group had longer hospital stay than lesser group. In addition, compared with lesser group, AKI and bacteremia were frequently developed in greater group. Our findings provide a rationale for using CE-CT scan as a tool for predicting clinical severity in patients with non-obstructive APN.
- APN is the most common form of upper urinary tract infection, and usually occurs secondary to an ascending infection of gram-negative bacteria in women.12 Although APN is easily treated by antibiotics, its clinical course and severity varies.1 Several risk factors are associated with the more severe presentations of urinary tract infection. Of these, urinary tract obstruction was independent predictor of septic shock.3,13 To evaluate urinary tract obsctrution due to various causes, radiological tests including CT or ultrasound are needed. In case of non-obstructive APN, the most common radiologic CT finding is a striated or wedge-shaped area of hypoperfusion or mass-like lesion after contrast injection.7,8 However, there are few data about such CT finding as a marker reflecting APN severity.7,8,14
- Paick et al. graded APN into 4 groups according to the extent of renal involvement; no renal parenchymal involvement as grade 1; less than 25% involvement as grade 2; 25% to 50% involvement as grade 3; and greater than 50% as grade 4, and reported clinical usefullnes of CT grade for predicting clinical course of APN.14 In presenting study, we classified the subjects into two groups based on modification of method reported by Paick et al. Initially, we also classified the subjects into four groups according to APN grade reported by Paick et al, however, there were no statistically signficant differences among groups (the data were not shown). This finding migth be due to the difference of enrolled participants. In the study by Paick et al, the mean age of the study population was 39.3 years and there were no patients with AKI. On the other hand, the mean age in our study was 55.2 years, and the overall incidence of AKI was 14.5%. Thus, large prospective randomized controlled study is needed to check whether the assocation of the extent of renal involvment in CT and clinical severity can differ based on renal function. However, the increase in hospital stay of greater group, which is shown in our study, was also observed in the study reported by Paick et al.
- Urothelial thickening, diffuse peritoneal thickening, perinephric fat infiltration and the presence of two or more abonormal CT findings were more frequently observed in patients with bacteremic APN.15 However, there are few data about correation between bacteremia and extent of renal involvement.16 In case of patients with APN, blood cultures have been reported to be positive in 18–32% of APN cases.16–18 In our study, 158 (29.4%) patients out of 537 have positive blood culture, and bacteremia (36.4% vs 26.9%, P < 0.05) were frequently developed in greater group. During treatment of APN, it is important to differentiate bacteremic urinary tract infection (UTI) patients from non-bacteremic UTI patients since complication of bacteremic UTI can lead to sepsis or death. Thus, our data show that CT finding may be helpful to predict bacteremia in patients with APN.
- Old age, arteriosclerosis, diabetic vasculopathy, chronic hypertension, and chronic kidney disease are regarded as risk factors for renal failure due to impairment of the vasodilatory response in the afferent arteriole.19,20 In our study population, old age and 50% or greater renal parenchymal involvement in CT examination were significant risk factors for predicting APN-associated AKI. In this study, all patients with AKI recovered without renal replacement therapy after appropriate antibiotics and supporive care. According to our data, CT finding could be helpful to predict AKI in APN patients with preserved renal function.
- Our study had certain limitations. First, this was a retrospective single center study. Thus, a large, prospective, randomized, controlled multicenter study is needed in the future. Second, the subjects in present study had relativley preserved renal function since patients with poor renal function did not undergo CE-CT due to CI-AKI. Third, although several CT findings were observed in APN,15 we only investigated renal parenchymal involvement in CT. Thus, a large study using various CT findings in APN patients is needed in the future.
- In our study, the patients with 50% or greater renal parenchymal involvement in CE-CT had severe type of APN based on hospital stay, prsence of bacteremia and AKI. Therefore, CE-CT could be helpful to discriminate patients with severe from non-severe APN patients in non-obstructive patients with preserved renal function.
DISCUSSION
Fig. 1Acute pyelonephritis grades according to CT findings. (A) lesser grade, lesser than 50% of renal involvement (B) greater grade, greater than 50% of renal involvement.
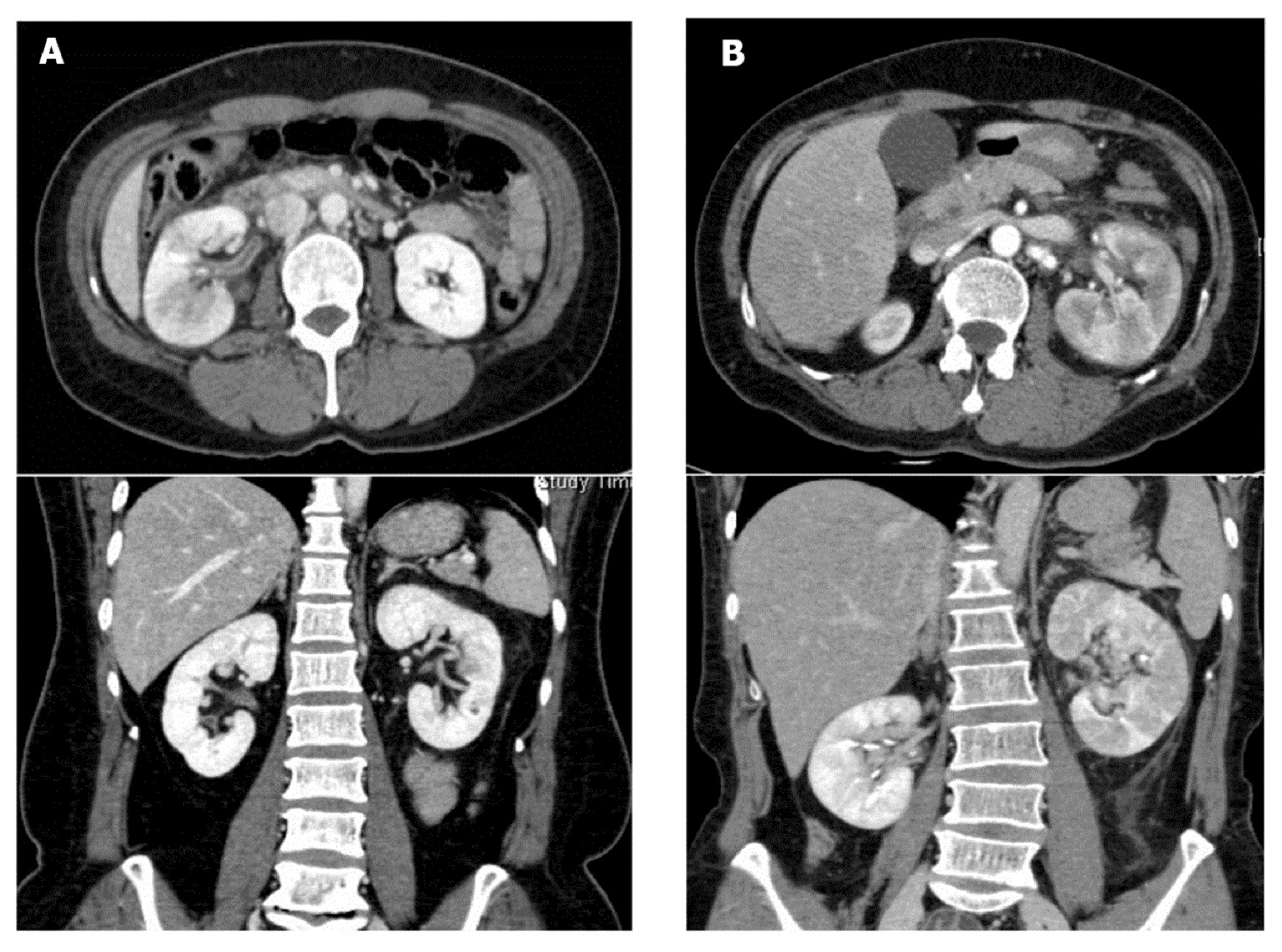
Table 1The clinical and laboratory findings of the 537 patients with nonobstructive acute pyelonephritis
Table 2Comparison of baseline characteristics between non-AKI and AKI group
Table 3Predictors of development of AKI (univaritive and multivariative analysis)
- 1. Bass PF 3d, Jarvis JA, Mitchell CK. Urinary tract infections. Prim Care 2003;30:41–61.ArticlePubMed
- 2. Nicolle LE. Urinary Tract infection. Crit Care Clin 2013;29:699–715.ArticlePubMed
- 3. Lee JH, Lee YM, Cho JH. Risk factors of septic shock in bacteremic acute pyelonephritis patients admitted to an ER. J Infect Chemother 2012;18:130–3.ArticlePubMed
- 4. Marschall J, Zhang L, Foxman B, Warren DK, Henderson JP. CDC Prevention Epicenters Program. Both host and pathogen factors predispose to Escherichia coli urinary-source bacteremia in hospitalized patients. Clin Infect Dis 2012;54:1692–8.ArticlePubMedPMC
- 5. Rabushka LS, Fishman EK, Goldman SM. Pictorial review: computed tomography of renal inflammatory disease. Urology 1994;44:473–80.ArticlePubMed
- 6. Kim JS, Lee S, Lee KW, Kim JM, Kim YH, Kim ME. Relationship between uncommon computed tomography findings and clinical aspects in patients with acute pyelonephritis. Korean J Urol 2014;55:482–6.ArticlePubMedPMC
- 7. Soluen MC, Fisherman EK, Goldman SM, Gatewood OM. Bacterial renal infection: role of CT. Radiology 1989;171:703–7.ArticlePubMed
- 8. Gold RP, McClennan BL, Rottenberg RR. CT appearance of acute inflammatory disease of the renal interstitium. AJR Am J Roentgenol 1983;141:343–9.ArticlePubMed
- 9. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract 2012;120:c179–84.ArticlePubMed
- 10. Kim MH, Koh SO, Kim EJ, Cho JS, Na SW. Incidence and outcome of contrast-associated acute kidney injury assessed with Risk, Injury, Failure, Loss, and End-stage kidney disease (RIFLE) criteria in critically ill patients of medical and surgical intensive care units: a retrospective study. BMC Anesthesiol 2015;15:23.ArticlePubMedPMC
- 11. Levey AS, Coresh J, Greene T, Marsh J, Stevens LA, Kusek JW, et al. Expressing the Modification of Diet in Renal Disease Study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin Chem 2007;53:766–72.ArticlePubMed
- 12. Ki M, Park T, Choi B, Foxman B. The epidemiology of acute pyelonephritis in South Korea, 1997–1999. Am J Epidemiol 2004;160:985–93.ArticlePubMed
- 13. Leligdowicz A, Dodek PM, Norena M, Wong H, Kumar A, Kumar A, et al. Association between source of infection and hospital mortality in patients who have septic shock. Am J Respir Crit Care Med 2014;18(9):1204–13.Article
- 14. Paick SH, Choo GY, Baek M, Bae SR, Kim HG, Lho YS, et al. Clinical value of acute pyelonephritis grade based on computed tomography in predicting severity and course of acute pyelonephritis. J Comput Assist Tomogr 2013;37:440–2.ArticlePubMed
- 15. Yu TY, Kim HR, Hwang KE, Lee JM, Cho JH, Lee JH. Computed tomography findings associated with bacteremia in adult patients with a urinary tract infection. Eur J Clin Microbiol Infect Dis 2016;35:1883–7.ArticlePubMed
- 16. Oh SJ, Je BK, Lee SH, Choi WS, Hong D, Kim SB. Comparision of computed tomography findings between bacteremic and nonbacteremic acute pyelonephritis due to Escherichia coli. World J Radiol 2016;28(4):03–9.
- 17. Lee H, Lee YS, Jeong R, Kim YJ, Ahn S. Predictive factors of bacteremia in patients with febrile urinary tract infection: an experience at a teritary care center. Infection 2014;42:669–74.ArticlePubMed
- 18. Kim KS, Kim K, Jo YH, Kim TY, Lee JH, Lee SJ, et al. A simple model to predict bacteremia in women with acute pyelonephritis. J Infect 2011;63:124–30.ArticlePubMed
- 19. Macedo E, Mehta RL. Prerenal failure: from old concepts to new paradigms. Curr Opin Crit Care 2009;15:467–73.ArticlePubMedPMC
- 20. Blantz RC, Singh P. Analysis of the Prerenal Contributions to Acute Kidney injury. Contrib Nephrol 2011;174:4–11.ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite