KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 30(2); 2015 > Article
-
Original Article
Analysis of an EGFR mutation by PNA clamping method in lung carcinoid tumors - Jong In Kim
-
Kosin Medical Journal 2015;30(2):141-147.
DOI: https://doi.org/10.7180/kmj.2015.30.2.141
Published online: January 20, 2015
Department of Thoracic and Cardiovascular Surgery, College of Medicine, Kosin University, Busan, Korea.
- Corresponding Author: Jong In Kim, Department of Thoracic and Cardiovascular Surgery, College of Medicine, Kosin University, 262, Gamcheon-ro, Seo-gu, Busan 49267, Korea. TEL: +82-51-990-6253 FAX: +82-51-990-3994 E-mail: schoi@ns.kosinmed.or.kr
• Received: October 21, 2014 • Accepted: April 1, 2015
Copyright © 2015 Kosin University School of Medicine Proceedings
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,050 Views
- 2 Download
- 2 Crossref
Abstract
-
Background
- Pulmonary carcinoid tumors consisting of typical carcinoid tumors (TC) and atypical carcinoid tumors (AC) are rare, accounting for 2–5% of all lung tumors. TC is considered a low-grade tumor with a rate of distant metastasis up to 12%. In contrast, ACs are more aggressive tumors, displaying a metastatic rate up to 70%. Surgery is the treatment of choice; however, the current treatment outcomes of metastatic lung carcinoids are discouraging. This study aimed to investigate the EGFR mutation using the PNA-mediated clamping method and to provide basic data for using EGFR-TK1 and its clinical implications.
-
Materials and Methods
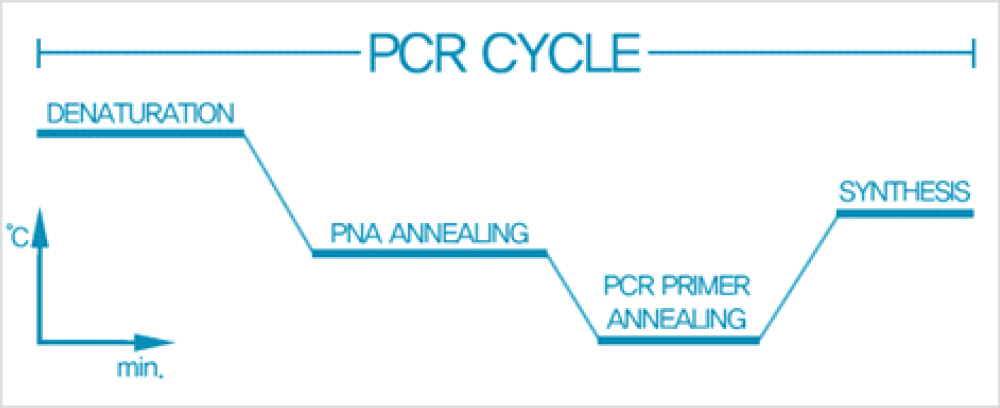
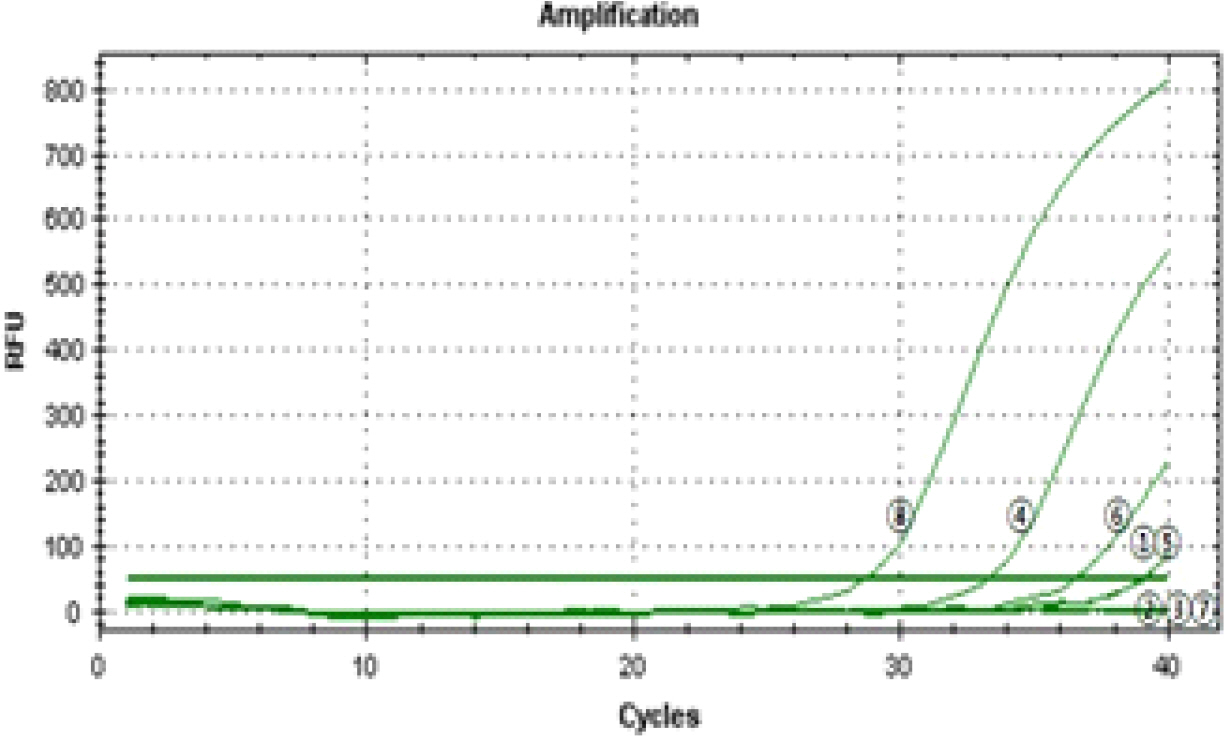
- A total of 14 cases that underwent surgery were diagnosed as carcinoid tumors and pathologically classified as TC and AC. The paraffin-embedded tissues were analyzed for EGFR mutations using the PNA-mediated PCR clamping technique. The mutant type was noted in the cases with a△Ct greater than 2.0.
-
Result
- Of 14 cases, eight were AC and six cases were TC. No known EGFR mutation was detected with a△Ct less than 2.0.
-
Conclusion
- The EGFR genotype determined using the PNA-mediated PCR clamping method was wild-type in all pulmonary carcinoid tumors. Therefore, the application of EGFR-TK1 is limited in pulmonary carcinoid tumors.
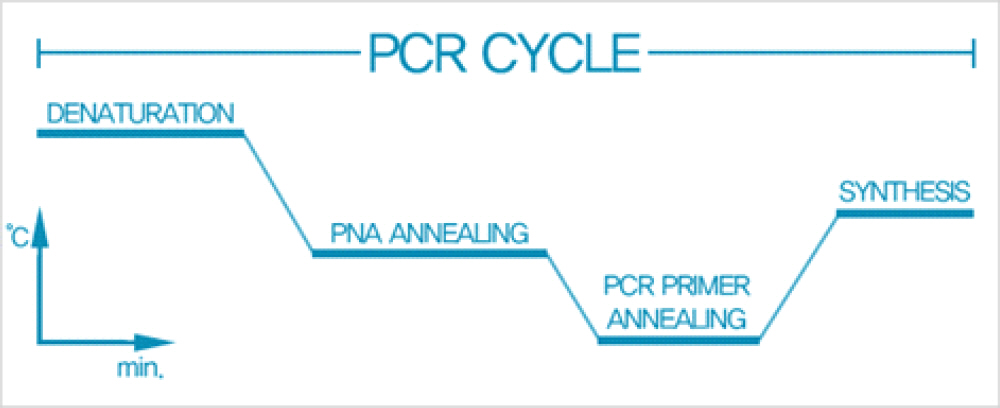
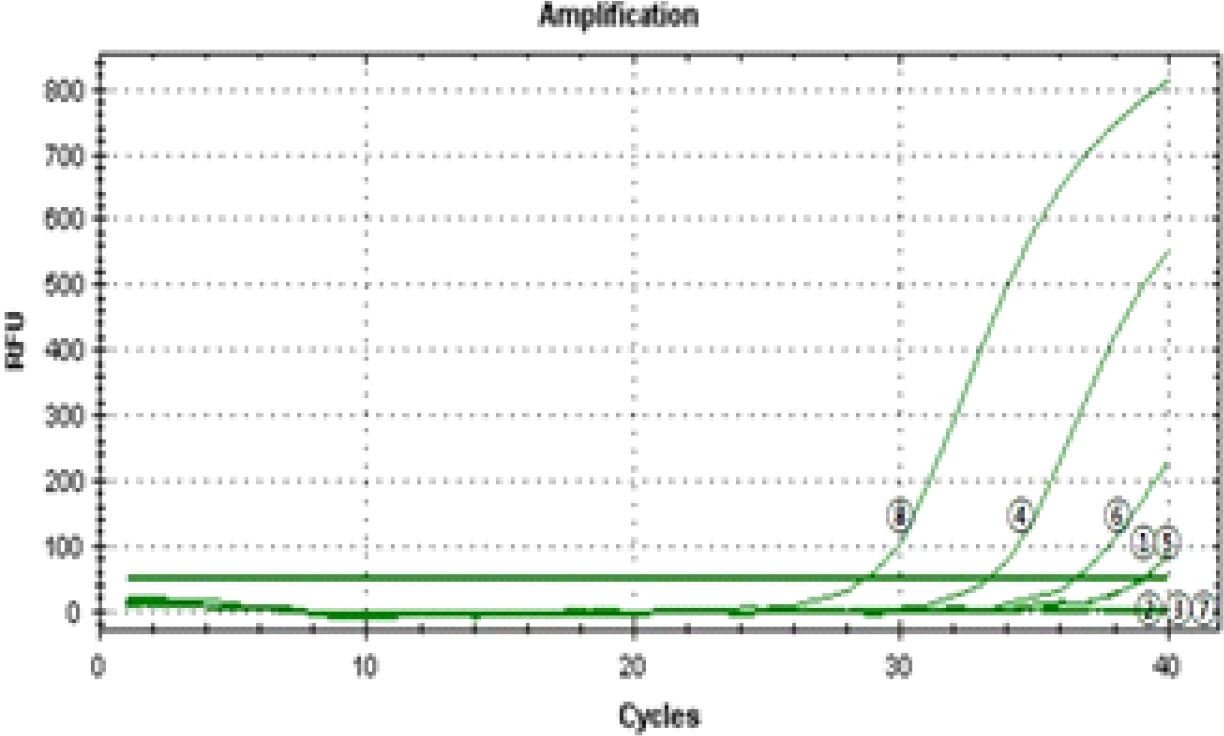
Table 1.The clinical and pathological characteristics of 14 cases of pulmonary carcinoid tumors
Table 2.The results of analysis of EGFR PNA-mediated clamping using real-time PCR
- 1. Cardillo G, Sera F, Di Martino M. Bronchial carcinoid tumors: nodal status and longterm survival after resection. Ann Thorac Surg 2004;77:1781–5.ArticlePubMed
- 2. Travis WD, Gal AA, Colby TV, Klimstra DS, Falk R, Koss MN. Reproducibility of neuroendocrine lung tumor classification. Hum Pathol 1998;29:272–9.ArticlePubMed
- 3. Kelly K, Huang C. Biological agents in non-small cell lung cancer: a review of recent advances and clinical results with a focus on epidermal growth factor receptor and vascular endothelial growth factor. J Thorac Oncol 2008;3:664–73.ArticlePubMed
- 4. Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med 2004;350:2129–39.ArticlePubMed
- 5. Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science 304:1497–500. 2004.ArticlePubMed
- 6. Thatcher N, Chang A, Parikh P, Rodrigues Pereira J, Ciuleanu T, von Pawel J, et al. Gefitinib plus best supportive care in previously treated patients with refractory advanced non-small-cell lung cancer: results from a randomised, placebocontrolled, multicentre study (Iressa Survival Evaluation in Lung Cancer). Lancet 366:1527–37. 2005.ArticlePubMed
- 7. Tsao MS, Sakurada A, Cutz JC, Zhu CQ, Kamel-Reid S, Squire J, et al. Erlotinib in lung cancer – molecular and clinical predictors of outcome. N Engl J Med 2005;353:133–44.ArticlePubMed
- 8. Zhu CQ, da Cunha Santos G, Ding K, Sakurada A, Cutz JC, et al. National Cancer Institute of Canada Clinical Trials Group Study BR.21. Role of KRAS and EGFR as biomarkers of response to erlotinib in National Cancer Institute of Canada Clinical Trials Group Study BR.21. J Clin Oncol 2008;26:4268–75.PubMed
- 9. Dacic S. EGFR assays in lung cancer. Adv Anat Pathol 2008;15:241–7.ArticlePubMed
- 10. Pao W, Ladanyl M. Epidermal growth factor receptor mutation testing in lung cancer: searching for the ideal method. Clin Cancer Res 2007;13:4954–5.ArticlePubMed
- 11. Lee KY. Molecular diagnosis in Lung Cancer. J Lung Cancer 2010;9:9–14.Article
- 12. Jang TW, Oak CH, Chang HK, Suo SJ, Jung MH. EGFR and KRAS mutations in patients with adenocarcinoma of the lung. Kor J Int Med 2009;24:48–54.Article
- 13. Saijo N, Fukuoka M, Thongprasert S, Ichinose Y, Mitsudomi T, Mok TS, et al. Lung cancer working group report. Jpn J Clin Oncol 2010;40:i7–12.ArticlePubMed
- 14. Tanaka T, Matsuoka M, Sutani A, Gemma A, Maemondo M, Inoue A. Frequency of and variables associated with the EGFR mutation and its subtypes. Int J Cancer 2010;126:651–5.ArticlePubMed
- 15. Kim HJ, Lee KY, Kim YC, Lee SY, Jang TW, Lee MK, et al. Detection and comparison of peptide nucleic acid-mediated real time polymerase chain reaction clamping and direct gene sequencing for epidermal growth factor receptor mutations in patients with non-small cell lung cancer. Lung cancer 2012;75:321–5.ArticlePubMed
- 16. Yeo CD, Kim JW, Kim KH, Ha JH, Rhee CK, Kim SJ, et al. Detection and comparison of EGFR mutation in matched tumor tissues, cell blocks, pleural effusions, and sera from patients with NSCLC with malignant pleural effusion, by PNA clamping and direct sequencing. Lung Cancer 2013;81:207–12.ArticlePubMed
- 17. Rickman OB, Vohra PK, Sanyal B, Vrana JA, Aubry MC, Wigle DA, et al. Analysis of ErbB receptors in pulmonary carcinoid tumors. Clin Cancer Research 2009;15:3315–24.Article
- 18. Wheler JJ, Falchook GS, Tsimberidou AM, Hong DS, Naing A, Piha-Paul SA, et al. Aberrations in the epidermal growth factor receptor gene in 958 patients with diverse advances tumors: implications for therapy. Ann Oncol 2013;24:838–42.PubMed
- 19. Gilbert JA, Lloyd RV, Ames MM. Lack of mutations in EGFR in gastroenteropancreatic neuroendocrine tumors. N Engl J Med 2005;353:209–10.ArticlePubMed
- 20. Ameur N, Lacroix L, Motte N, Baudin E, Caillou B, Ducreux M, et al. Mutational status of EGFR, BRAF, PI3KCA and JAK2 genes in endocrine tumors. Int J Cancer 2009;124:751–3.PubMed
- 21. Jackman DM, Yeap BY, Sequist LV, Linderman N, Holmes AJ, Joshi VA. Exon 19 deletion mutation of EGFR are associated with prolonged survival in non-small cell lung cancer patients treated with gefitinib or erlotinib. Clin Cancer Res 2006;12:3908–14.ArticlePubMed
- 22. Thomas CF Jr, Tazelaar HD, Jett JR. Typical and atypical pulmonary carcinoids outcome in patients presenting with regional lymph node involvement. Chest 2001;119:1143–50.PubMed
- 23. Yanagisawa S, Morikawa N, Kimura Y, Nagano Y, Murakami K, Tabata T. Large cell neuroendocrine carcinoma with epidermal growth factor receptor mutation: possible transformation of lung adenocarcinoma. Respirology 2012;17:1275–7.PubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Lung NETs and GEPNETs: One Cancer with Different Origins or Two Distinct Cancers?
Georgios Evangelou, Ioannis Vamvakaris, Anastasia Papafili, Maximilian Anagnostakis, Melpomeni Peppa
Cancers.2024; 16(6): 1177. CrossRef - STAT3 inhibition decreases ATP-induced MUC8 gene expression in human airway epithelial cells
Cheol Hong Kim, Kyoung Seob Song
Kosin Medical Journal.2022; 37(2): 134. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite