KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 29(1); 2014 > Article
-
Original Article
Characteristics of Peripheral versus Central Lung Cancer Since 2000 - So Young Ock, Tae Won Jang, You Jin Han, Go Eun Yeo, Eun Jung Kim, Won Hyoung Lee, Nam Kyu Kim
-
Kosin Medical Journal 2014;29(1):47-52.
DOI: https://doi.org/10.7180/kmj.2014.29.1.47
Published online: December 17, 2014
Department of Internal Medicine, College of Medicine, Kosin University, Busan, Korea
- Corresponding Author: So Young Ock, Deparment of Internal Medicine, College of Medicine, Kosin University, 34 Amnamdong, Seo-gu, Busan, 602-702, Korea TEL: +82-51-990-6460 FAX: +82-51-990-3049 E-mail: oaksoyoung@naver.com
• Received: July 30, 2013 • Revised: February 8, 2014 • Accepted: February 12, 2014
Copyright © 2014 Kosin University School of Medicine Proceedings
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,270 Views
- 4 Download
- 1 Crossref
Abstract
-
Objectives
- The aim of this study was to explore the changes of bronchoscopic features according to epidemiologic change of lung cancer.
-
Methods
- We performed a retrospective review of the clinical characteristics of 1,139 lung cancer patient who underwent bronchoscopy at Kosin University Hospital from January 2000 to December 2010.
-
Results
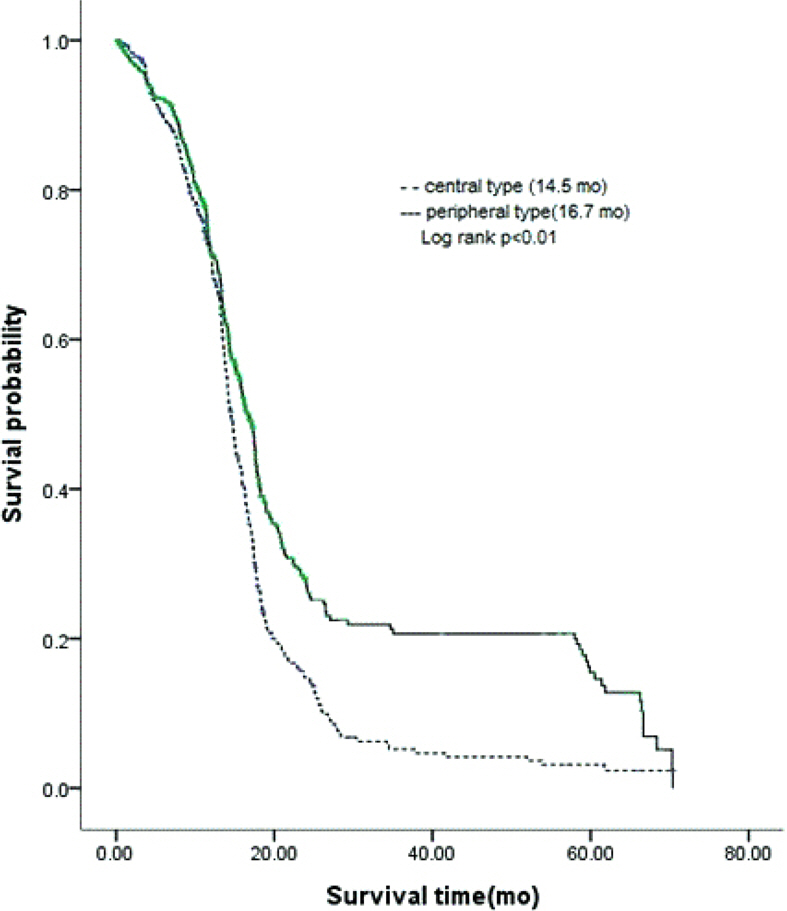
- The age of patients increased significantly during the last decade (P < 0.001). The most common histological type was adenocarcinoma (38.1%), followed by squamous carcinoma (35.7%) and small cell carcinoma (15.3%). There was an increasing incidence of adenocarcinoma over the time (P < 0.001). Bronchoscopic feature were divided into two classes; central type, peripheral type. The peripheral type was predominant (62.3%). The proportion of peripheral type has been increased in process of time (49.7% vs. 63.7% vs. 73.7%; P < 0.01). Among the major histopathologic type of lung cancer, adenocarcinoma (81.3%) and unclassifiable non-small-cell lung cancer (73.4%), small cell carcinoma (56.9%) were associated with preferential occurrence of peripheral type. Squamous cell carcinoma of the lung more often arised in central type (59%). However, the proportion of peripheral squamous cell carcinoma has been increased. On the subgroup analysis, the median survival time of peripheral type with adenocarcinoma and small cell carcinoma were longer than central type (P < 0.05).
-
Conclusions
- The age of the lung cancer patients at diagnosis was getting older. The most frequent histopathologic type was adenocarcinoma. The proportion of peripheral type lung cancer gradually increased over the time. The survival time of peripheral type lung cancer was longer than central type.
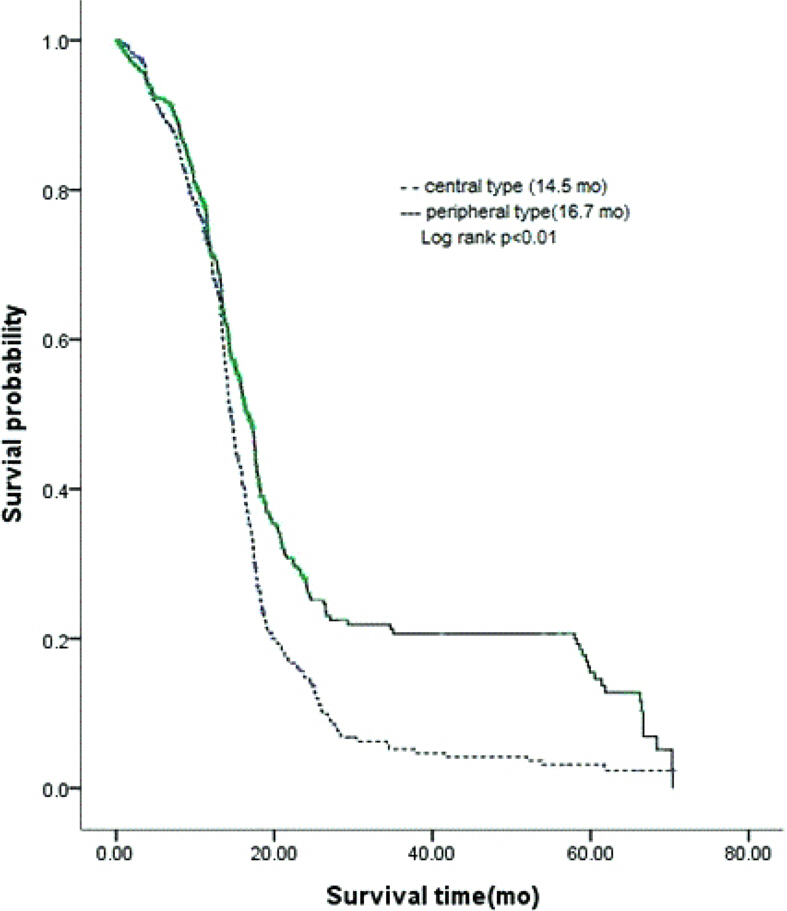
Table 1.Patient characteristics
Table 2.Annual trends of clinical characteristics of lung cancer in Kosin University
Table 3.Comparison clinical characteristics central type lung cancer with periphera lung cancer
- 1. Korean National Statistical Office, Annual Report on the Cause of Death Statistics. Korea National Statistical Office 2006.
- 2. Travis WD, Travis LB, Devesa SS. Lung cancer. Cancer 1995;75:191–202.ArticlePubMed
- 3. Kim YC, Kwon YS, Oh IJ, Kim KS, Kim SY, Ryu JS, et al. National survey of lung cancer in Korea, 2005. J Lung Cancer 2007;6:67–73.Article
- 4. Lim JH, Ban HJ, Oh IJ, Kim SO, Son JG, Jeong JP, et al. Clinical characteristics of lung cancer diagnosed in Chonnam National University Hospital (CNUH) since 2000. Tuberc Respir Dis 2006;61:427–32.Article
- 5. Brooks DR, Austin JH, Heelan RT, Ginsberg MS, Shin V, Olson SH, et al. Influence of Type of Cigarette on Peripheral versus Central Lung Cancer. Cancer Epidemiol Biomarkers Prev 2005;14:576–81.ArticlePubMed
- 6. Ugur G, Ibrahim A, Tanseli E. Classification of fibreoptic bronchoscopic findings: analysis of 2,698 cases. Comp Clin Path 2004;13:1–3.Article
- 7. Mountain CF. Revisions in the International System for Staging Lung Cancer. Chest 1997;111:1710–7.ArticlePubMed
- 8. Jackman DM, Johnson BE. Small-cell lung cancer. Lancet 2005;366:1385–96.ArticlePubMed
- 9. Thun MJ, Lally CA, Flannery JT, Calle EE, Flanders WD, Heath CW Jr. Cigarette smoking and changes in the histopathology of lung cancer. J Natl Cancer Inst 1997;89:1580–6.ArticlePubMed
- 10. Strauss GM, Jemal A, McKenna MB, Strauss JA, Cummings KM. The epidemic of smoking-related adenocarcinoma of the lung: The role of the tobacco industry and filtered and low-tar cigarettes: PRS-01. J Thorac Oncol 2007;2:S305.Article
- 11. Yu IT, Chiu YL, Au JS, Wong TW, Tang JL. Dose-response relationship between cooking fumes exposures and lung cancer among Chinese nonsmoking women. Cancer Res 2006;66:4961–7.ArticlePubMed
- 12. Bryd RB, Carr DT, Miller WE, Payne WS, Woolner LB. Radiographic abnormlities in carcinoma of the lung as related to histological cell type. Thorax 1969;24:573–5.ArticlePubMedPMC
- 13. Lubin JH, Blot WJ, Berrino F, Flamant K, Gillis CR, Kunze M, et al. Patterns of lung cancer risk according to type of cigarette smoked. Int J Cancer 1984;33:569–76.ArticlePubMed
- 14. Yang CP, Gallagher RP, Weiss NS, Band PR, Thomas DB, Russell DA. Differences in incidence rates of cancers of the respiratory tract by anatomic subsite and histologic type: an etiologic implication. J Natl Cancer Inst 1989;81:1828–31.ArticlePubMed
- 15. Wynder EL, Muscat JE. The changing epidemiology of smoking and lung cancer histology. Environ Health Perspect 1995;103:143–8.Article
- 16. Huhti E, Saloheimo M, Sutinen S, Reinilä A. Does the location of lung cancer affect its prognosis? Eur J Respir Dis 1983;64:460–5.PubMed
- 17. Jang TW, Kim YC, Kwon YS, Oh IJ, Kim KS, Kim SY, et al. Female lung cancer: Re-analysis of national survey of lung cancer in Korea, 2005. J lung cancer 2010;9:57–63.Article
- 18. Tomashefski JF Jr, Connors AF Jr, Rosenthal ES, Hsiue IL. Peripheral vs central squamous cell carcinoma of the lung. A comparison of clinical features, histopathology, and survival. Arch Pathol Lab Med 1990;114:468–74.PubMed
- 19. Ketchedjian A1. Daly BD, Fernando HC, Florin L, Hunter CJ, Morelli DM, et al. Location as an important predictor of lymph node involvement for pulmonary adenocarcinoma. J Thoracic Cardiovasc Surg 2006;132:544–8.Article
References
Figure & Data
References
Citations
Citations to this article as recorded by 
- Ablation of Liver X receptors α and β leads to spontaneous peripheral squamous cell lung cancer in mice
Yu-bing Dai, Yi-fei Miao, Wan-fu Wu, Yu Li, Francesca D'Errico, Wen Su, Alan R. Burns, Bo Huang, Laure Maneix, Margaret Warner, Jan-Åke Gustafsson
Proceedings of the National Academy of Sciences.2016; 113(27): 7614. CrossRef
 PubReader
PubReader Cite
Cite