KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 37(4); 2022 > Article
-
Original article
Students’ perceptions of the learning environment at a medical school in Korea: comparisons of the most recent 4 years’ results using the Dundee Ready Education Environment Measure (DREEM) -
Sejin Kim

-
Kosin Medical Journal 2022;37(4):299-310.
DOI: https://doi.org/10.7180/kmj.22.129
Published online: December 7, 2022
Department of Medical Education, Kosin University College of Medicine, Busan, Korea
- Corresponding Author: Sejin Kim, PhD Department of Medical Education, Kosin University College of Medicine, 262 Gamcheon-ro, Seo-gu, Busan 49267, Korea Tel: +82-51-990-6667 Fax: +82-51-241-5458 E-mail: sejintkim@gmail.com
Copyright © 2022 Kosin University College of Medicine.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,025 Views
- 18 Download
Abstract
-
Background
- The learning environment is an essential factor influencing students’ educational processes and personal quality of life. The purpose of this study was to examine medical students’ perceptions of the learning environment at a medical school over the most recent 4 years and explore possibilities for learning environment reform and revision based on the results.
-
Methods
- Participating students were asked about their perceptions of the learning environment using the Dundee Ready Education Environment Measure (DREEM) questionnaire, which was distributed to first-year, third-year, and fourth-year students, representing each learning period. In total, 349 students participated in this study. Analysis of variance was conducted to determine differences in DREEM scores among years and learning periods.
-
Results
- There were no statistically significant differences in DREEM scores by year and learning period, except for students’ perceptions of teachers and students’ perceptions of atmosphere. However, in an analysis of differences in DREEM scores in the class of 2018 cohort by learning period, four domains of the DREEM (except for students’ academic self-perceptions) and the total DREEM score were found to be significantly different.
-
Conclusions
- Students’ perceptions of the learning environment at Kosin University College of Medicine were relatively high. The total score increased from 2019 to 2022, except for 2021. Another significant result was that basic science students had the highest perceptions, whereas students in basic clinical science had the lowest perceptions. To improve the learning environment for medical students, continuing support for students’ emotional stability, learning motivation, physical environment, social relationships, and counseling is essential.
- The learning environment is one of the fundamental components influencing students’ educational processes [1,2] and personal quality of life [3,4]. Learning depends on academic experiences including the curriculum, teachers, students’ motivations, physical settings, and related interactions with peers and professors in the processes [2,5]. In addition, social interactions and psychological contexts play significant roles in students’ well-being [1]. The learning environment at a medical school comprises academic experiences that foster professional development as future physicians’ competencies [5-7] and contexts that influence students’ mental and physical quality of life to overcome academic failure tolerance as social issues [3,8,9]. Previous studies have reported that the learning environment can affect academic activities and performance, including all intended learning, informal learning from the hidden curricula, and student outcomes [5]. In particular, medical students suffer from stress including heavy workload, competition with classmates, and anxiety about future careers. They are rarely satisfied due to these pressures in the learning environment at a medical school [10]. However, students’ failure at medical school has been considered personal troubles or individual inability in Korea [9]. Therefore, measuring medical students’ perceptions of the learning environment is critical to identify and understand current situations in learning processes and students’ quality of life. It may allow institutions to improve their environment positively for students to acquire intended competencies continually and be supported by the school system.
- The Dundee Ready Education Environment Measure (DREEM) was designed and developed to evaluate students’ perceptions of the learning environment using a universal diagnostic inventory at medical schools [11]. It has also been used for other health professionals’ perceptions regarding the educational environment [12] and tested in different schools and countries for validation [13]. The DREEM is comprised of a total of 50 closed statements in five sub-factors: students’ perceptions of learning (SPL), students’ perceptions of teachers (SPT), students’ academic self-perceptions (SAS), students’ perceptions of atmosphere (SPA), and students’ social self-perceptions (SSS). Perceptions of each sub-factor from medical students regarding how they perceive the learning environment can be calculated and evaluated through this measuring tool. It has been utilized as an evaluation method to identify current insufficiencies in the learning environment in past years [13].
- Results of the DREEM have been reported in different countries and institutions for several years. Based on meta-analysis results regarding how the DREEM has been used, undergraduate medical students have commonly participated as target subjects. Purposes of previous studies could be classified into four categories: diagnostic, comparison with different groups, comparison with same groups, and relationship with other measures [13]. In particular, one research has examined medical students’ perceptions of the educational environment at medical schools in Korea through nationwide surveys using the DREEM [14]. It analyzed and reported scores of the overall mean and each sub-factor from 40 medical schools. It also compared the scores by educational systems, grades, genders, and academic achievement levels. However, there was no considerable follow-up study particularly comparing different groups in the same institution to analyze the current learning environment by years after the nationwide report in Korea. Therefore, the purpose of this study was to examine medical students’ perceptions of the learning environment at a medical school over the years and explore possibilities of learning environment reform and revision based on results of the learning environment analysis. In particular, this study was conducted to answer the following research questions: (1) what are the differences of medical students’ perceptions on the learning environment by years? (2) what are the differences of medical students’ perceptions on the learning environment by learning periods? and (3) what are the differences of medical students’ perceptions on the learning environment by cohorts? To achieve this purpose, medical school students were asked about their perceptions of the learning environment using the DREEM, a reliable and validated measuring tool.
Introduction
- Ethical statements: This study was approved by the Institutional Review Board (IRB) of Kosin University Gospel Hospital (IRB No. KUGH 2022-04-011). The requirement of informed consent was waived by the IRB because this research involved the secondary analysis of existing data already collected by Kosin University College of Medicine.
- 1. Research background
- Kosin University College of Medicine (KUCM) was a research site having 80 undergraduate students in each grade. Well-organized curricula based on four learning periods (basic science, basic clinical science, clinical medicine, and clinical practice) are provided to students to accomplish appropriate learning competencies relative to each period. The learning periods are classified according to each grade and semester; basic science period consists of the first grade (2 semesters), basic clinical science period consists of the second grade and the half of the third grade (3 semesters), clinical medicine period consists of the half of the third grade and the fourth grade (3 semesters), and clinical practice period consists of the fifth and sixth grades (4 semesters).
- KUCM has been trying to adopt competency-based medical education and an integrated curriculum. All professors are continually encouraged to deliver their learning contents with learner-centered classes, however, most courses are still teacher-centered with lecture-based teaching methods. Therefore, medical education-focused professors have been delegated to facilitate and utilize various teaching-learning methods. Moreover, the center for educational development and evaluation opened to monitor and evaluate the whole educational system in general and to design and develop a new curriculum based on evaluation results since 2020. For students’ mental health, the center for student health and counseling has been operating and providing various tests and counseling to students.
- KUCM has a total of 162 professors from basic clinical science and clinical science departments (including related medical education and medical humanities) who are teaching students. KUCM has sufficient physical facilities for students and faculty to ensure that learning activities can be delivered adequately. Independent school building is being operated with an affiliated hospital for students to have clinical experiences, including sufficient number and categories of patients, clinical training facilities, and supervision of clinical practices. The institutional autonomy of KUCM is guaranteed to design and implement the curriculum using allocated resources and budget.
- 2. Research participants
- The DREEM questionnaire was distributed to the first year, third year, and fourth year students representing each learning period of basic science, basic clinical science, and clinical medicine (except clinical practice). A total of 85, 155, 57, and 52 students responded in 2019, 2020, 2021, and 2022, respectively. A total of 349 students participated in this study. Detailed information regarding research participants including response rates and the number of students of each learning period in each year are provided in Table 1.
- 3. Data collection and statistical analysis
- DREEM data have been collected through an online survey form at KUCM since 2019. All data from the DREEM were self-reported, and students’ participation was voluntary. Results from the DREEM are utilized every year to improve the learning environment affecting students’ learning outcomes at KUCM. The DREEM survey is a part of educational monitoring system, operated by center for educational development and evaluation, and the results have been reported to the committee of quality improvement. The committee makes a plan to improve or upgrade inadequate parts in the learning environment. For example, center for student health and counseling keeps providing counseling programs for students, and conference rooms were renovated for small group discussions or individual studies. To collect more reliable data from participants, all identifying information except their grades were not collected. Additionally, the primary researcher strictly restricted access to collected data. In this study, the internal consistency of survey questions was very high (Cronbach α=0.956), and the internal consistency of each sub-factor of the DREEM was also relatively high (Table 2).
- One-way analysis of variance (ANOVA) was conducted to determine differences in DREEM scores among years and learning periods, respectively, and the differences were also analyzed by cohorts. In this study, most cohorts only had two data points: basic clinical science and clinical medicine or basic science and basic clinical science. On the other hand, the cohort for 2018 had three data points: basic science (32 participants), basic clinical science (19 participants), and clinical medicine (19 participants). Therefore, data for the class of 2018 were used for chronological analysis.
- p-value <0.05 was considered statistically significant in this study. Descriptive statistics including the mean and standard deviation were calculated. All quantitative analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Data from participating students who did not respond or had insincere responses were excluded from analysis. Some questions from the DREEM questionnaire were coded reversely for data analysis.
Methods
- Results of comparative analysis to identify students’ perceptions of the learning environment at KUCM are presented below by years, learning periods, and cohorts.
- 1. Results of DREEM scores by years
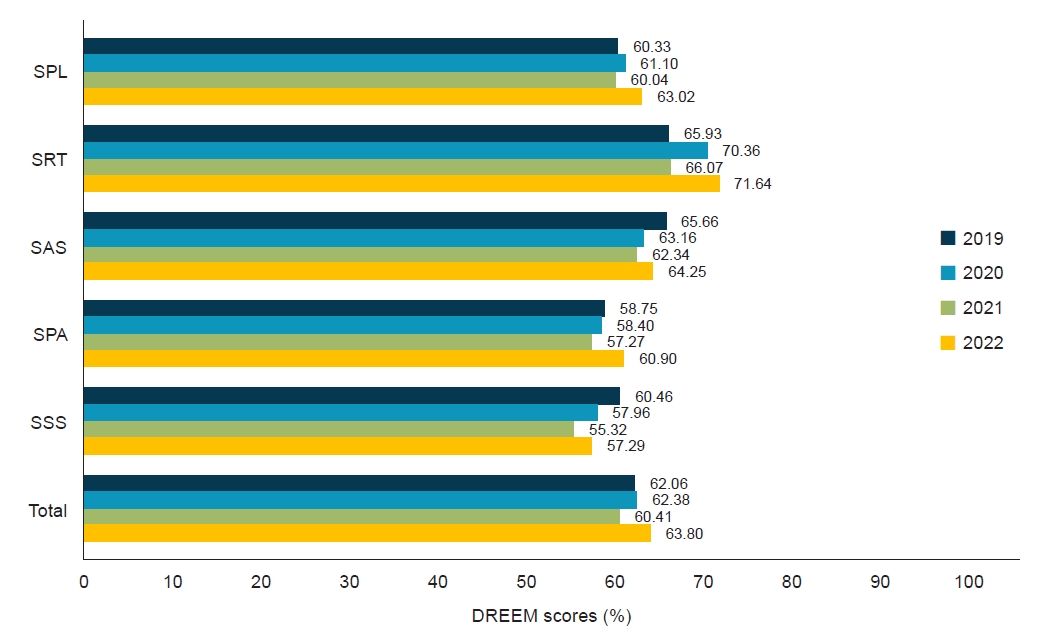
- Results of DREEM scores by years including total and each domain of DREEM scores were analyzed by one-way ANOVA. Results are displayed in Table 3 and Fig. 1. Total score of the DREEM was 124.12 (SD=23.12) in 2019, 124.75 (SD=24.83) in 2020, 120.82 (SD=26.34) in 2021, and 127.60 (SD=24.56) in 2022 (max=200). Scores from each domain of the DREEM are presented below by years from 2019 to 2022.
- To determine differences in DREEM scores by years, ANOVA was conducted. Results are presented in Table 4. Scores were compared for the five domains of the DREEM and the total score. However, there was no significant difference except for the domain of SPT (F=3.84, p=0.010).
- 2. Results of DREEM scores by learning periods
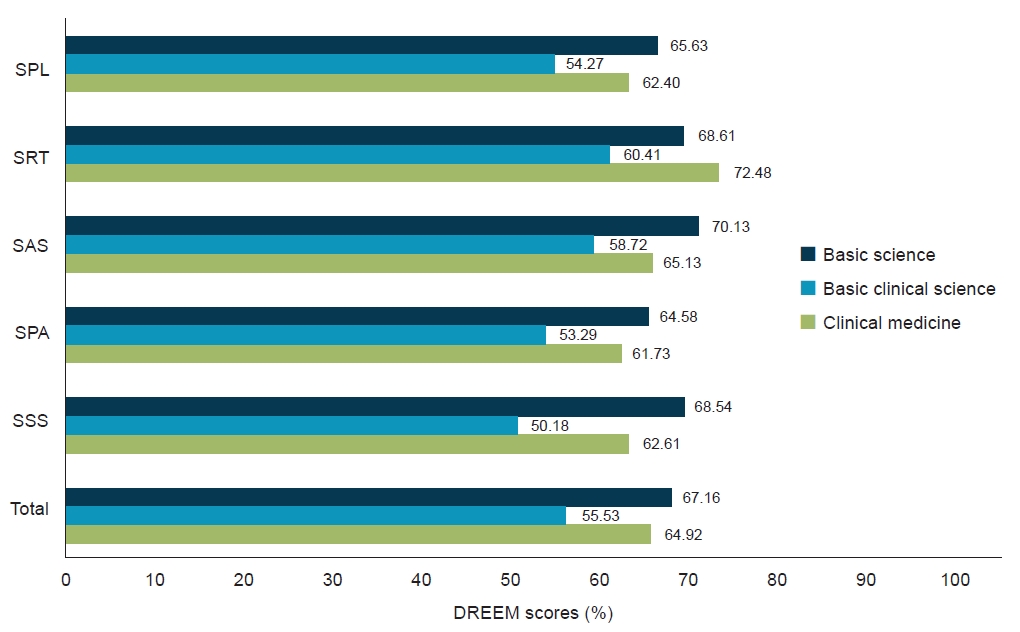
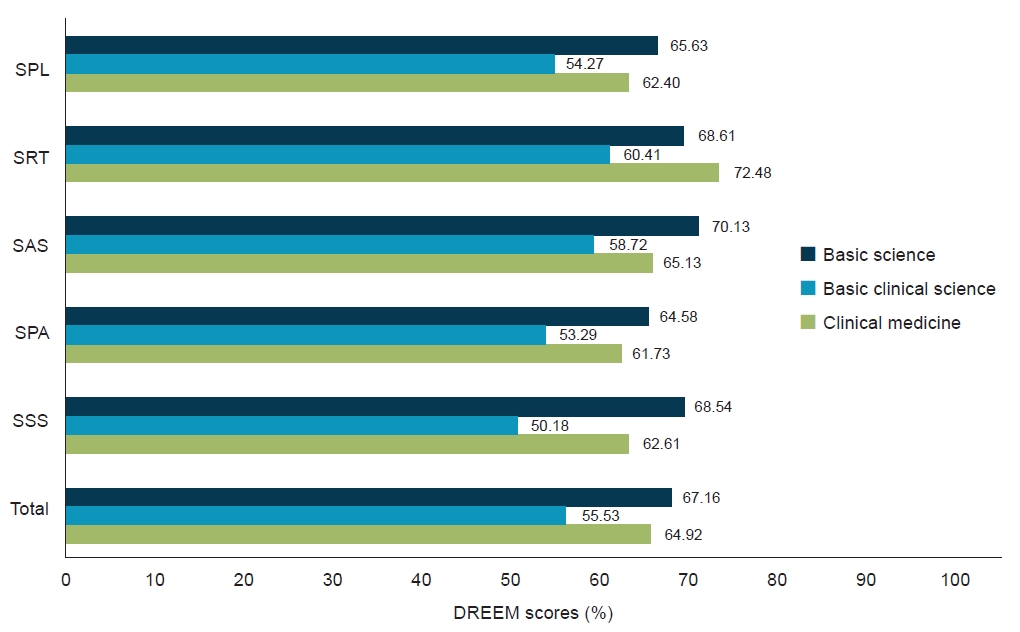
- Results of DREEM scores by learning periods including the total score and score for each domain of the DREEM were analyzed by one-way ANOVA. Results are displayed in Table 5 and Fig. 2. The total score of the DREEM was 127.26 (SD=25.85) for basic science, 121.40 (SD=24.75) for basic clinical science, and 124.03 (SD=23.30) for clinical medicine (max=200). Scores from each domain of the DREEM are presented below by learning periods.
- To determine differences in DREEM scores by learning periods, ANOVA was conducted. Results are presented in Table 6. Scores were compared for the five domains of the DREEM and the total score. However, there was no significant difference except for the domain of SPA (F=5.34, p=0.005).
- 3. Results of DREEM scores by cohorts
- Results of DREEM scores by cohorts from 2016 to 2019 including total score and each domain score of the DREEM were analyzed by one-way ANOVA. Results are displayed in Table 7 and Fig. 3. In this study, most cohort only had two data points: basic clinical science and clinical medicine or basic science and basic clinical science. On the other hand, the cohort for 2018 had three data points: basic science, basic clinical science, and clinical medicine. Therefore, data for the class of 2018 were used for chronological analysis. The total score of the DREEM for the class of 2018 was 134.31 (SD=21.12) in basic science, 111.05 (SD=27.56) in basic clinical science, and 129.84 (SD=30.05) in clinical medicine (max=200). Scores from each domain of the DREEM are presented below by learning periods.
- To determine differences in DREEM scores for the class of 2018 cohort by learning periods, ANOVA was conducted. Results are presented in Table 8. Scores for the five domains and total score of the DREEM showed statistically significant differences (F=3.39, p=0.040 for SPL; F=4.15, p=0.020 for SPT; F=4.78, p=0.012 for SPA; F=8.58, p=0.000 for SSS; and F=5.13, p=0.008 for total) except for the domain of SAS (F=2.84, p=0.066).
Results
- The purpose of this study was to investigate medical students’ learning environment perceptions regarding learning, teachers, academic self-perceptions, atmosphere, and social self-perceptions and explore possibilities of learning environment reform and revision based on results of the learning environment analysis using the DREEM. KUCM has been using the DREEM survey to evaluate the learning environment since 2019, and the cohort finished the survey this year and participated fully in the evaluation from the period of basic science to clinical medicine. For this reason, current research is necessary at this point to compare results of the DREEM for four years’ data consecutively. Therefore, a comparative study was performed for DREEM scores by years, learning periods, and cohorts, and analysis results revealed the following four key findings:
- First, students’ perceptions of the learning environment at KUCM were relatively high. The total score of the DREEM was 124.12 (SD=23.12) in 2019, 124.75 (SD=24.83) in 2020, 120.82 (SD=26.34) in 2021, and 127.60 (SD=24.56) in 2022. These results can be interpreted as “more positive than negative” (101–150). Each year’s result was higher than 113.97 (SD=21.59), the average of 40 medical schools in Korea reported in 2015, and these results are at the high rank of 40 medical schools [14].
- However, total scores are still not comparable to those of other medical schools in Europe, such as school of medicine, at the University of Dundee, which has a learner-centered and integrated curriculum, problem-based learning, and efforts for developing a better learning environment [15]. As mentioned by Park et al. [14], the learning environment of medical schools still has some room for improvement. In particular, results from KUCM showed that SPA and SSS domain scores were relatively lower than those of other domains. One of the DREEM questions is “there is a good support system for students who get stressed,” and the scores from recent four years for this question were below 2.0 out of 4.
- To overcome these weaknesses, continuous support for students’ emotional stability, learning motivation, physical environment, social relationship, and counseling is essential. For example, operating the center for SHAC is a good starting point for improving the learning environment. Various counseling programs, including Minnesota Multiphasic Personality Inventory-2 for freshmen, Begin Again for returning students, and career counseling, have been provided for students who are willing to participate, and the satisfaction level of those programs were relatively high.
- Second, based on results of the DREEM by years, the total score increased from 2019 to 2022 except for 2021. Since total scores were not statistically different (F=0.69, p=0.559), indicating that the learning environment at KUCM was getting better. Also, the lowest result in 2021 was affected by coronavirus disease (COVID-19) because most students attended their classes through the online platform.
- Scores for the five sub-domains of the DREEM were compared by years. Only the domain of SPT showed a statistically significant difference (F=3.84, p=0.010). This was because every professor was forced to upload learning materials before the classes based on students’ opinions and program evaluation reports. Therefore, students were able to utilize materials in classes. Moreover, because students may trust their professors’ teaching and abilities for them to learn properly, the SPT has been better than other domains. On the other hand, the domain of SSS was getting lower since 2019, although there was no statistically significant difference (F=1.25, p=0.291). Various studies have reported that medical students experience both personal distress (quality of life and depression) and professional distress (burnout) more than other college students [3,16,17]. In particular, the COVID-19 situation in 2020 affected students’ mental and physical distances which critically increased their stress levels. It is not fully recovered by 2022. Kim et al. [18] have mentioned that emotional exhaustion can be both a starting point and a tipping point to arouse students’ burnout syndrome.
- To overcome this suffering, supporting students to control their stress levels and learning pressures is necessary [19]. For example, a mentor-mentee program or operating a counseling system by professionals can be helpful for students to manage their difficulties. Providing elective courses regarding self-regulation and time management, or stress relief programs during the basic science period is also meaningful.
- Third, based on results of the DREEM by learning periods, the total score was 127.26 (SD=25.85) for basic science, 121.40 (SD=24.75) for basic clinical science, and 124.03 (SD=23.30) for clinical medicine. All five sub-domains of the DREEM from the period of basic clinical science had the lowest scores among learning periods, although these scores were not significantly different except for the domain of SPA (F=5.34, p=0.005). This result may differ from the result that 4th-year (in clinical medicine at KUCM) students’ perceived scores for the learning environment were the lowest in the previous research [14]. The reason was that students begin to take classes related to clinical science and clinical medicine after they pass basic science subjects, including chemistry and biology through the basic clinical science period. Students experience academic pressures and extreme stress from the learning period caused by the amount of learning and anxiety from failure [16]. Moreover, most students in the period of basic clinical science addressed that the learning atmosphere of the school was not enough for them to feel comfortable or receive learning motivation to study in a short period of time. Students during the basic clinical science period are in the stage of adjusting and managing their time and effort, learning strategies, and stress relief. Therefore, satisfaction is relatively lower in the learning environment than in other learning periods.
- To provide a better learning environment for students in the basic clinical science period, redesigning the teaching and learning process to avoid teacher-centered classes, including rote memorization based on a short-term memory from certain subjects, is essential. Based on individual questions from the DREEM, including “The teaching over-emphasizes factual learning (negative item),” “The teaching encourages me to be an active learner,” and “Long-term learning is emphasized over short-term learning,” the scores of those items were relatively lower than other items. Therefore, providing more opportunities for students to think critically to solve problems through their own knowledge, and understanding based on the basic clinical science mechanism can allow students to receive more learning motivation to study basic clinical science as a foundation for clinical medicine. For example, meaningful learning can be provided through an integrated curriculum using clinical cases between basic clinical science and clinical medicine. Problem-based learning method is also an alternative learning strategy for enhancing students’ critical thinking. Flipped learning can provide more time for students to manage their time and effort to obtain content knowledge and for professors to orchestrate an integrated curriculum for meaningful learning sessions.
- Fourth, based on results of the DREEM for the class of 2018 cohort by learning periods, the total score was 134.31 (SD=21.12) for the basic science period in 2018, 111.05 (SD=27.56) for the basic clinical science period in 2020, and 129.84 (SD=30.05) for the clinical medicine period in 2022. Their differences were statistically significance (F=5.13, p=0.008). Scores of sub-domains were also found to be statistically different, except for the domain of SAS (F=3.39, p=0.040 for the SPL; F=4.15, p=0.020 for the SPT; F=4.78, p=0.012 for the SPA; and F=8.58, p=0.000 for the SSS). Results of the DREEM for the class of 2018 cohort had similar patterns, with scores being the highest for the basic science period and the lowest for the basic clinical science period. For domains of SPL, SPA, and SSS, students during the basic science period were relatively satisfied with the learning environment. Their satisfaction levels were then decreased within 1 year by more than 10% (from 65.63% to 54.27% for SPL, from 64.58% to 53.29% for SPA, and from 68.54% to 50.18% for SSS). After they passed the basic clinical science period, scores then increased and recovered during the clinical medicine period, although they were still not as high as scores during the basic science period. Trends of scores’ changes showed the current situation regarding the learning environment at KUCM. As mentioned above, considering various teaching methods utilized to enhance students’ clinical reasoning and problem-solving abilities and providing meaningful learning sessions are critical.
- This study provides meaningful and useful information including differences in years, learning periods, and cohorts on medical students’ perceptions of the learning environment through the DREEM at KUCM as a case study. Although a meaningful and useful research was done, this study has some limitations. First, only students’ perceived data were used for this study. There might be differences between students’ ideal perceptions and actual perceptions. Second, generalization of results from this study is limited by the research method, a case study. Results of the DREEM from one medical school could not be guaranteed to be applied to other medical schools. However, most medical schools in Korea have similar curricula and student populations. Thus, the results of this study might be useful for other schools to compare differences indirectly.
- The importance of the learning environment for medical students to learn properly is now undeniable. Human components of the learning environment, such as learning, teacher, academic self-perceptions, atmosphere, and social relationships, are also important as much as the physical environment. As a result, collecting and analyzing consecutive results of the DREEM is essential because external factors, such as the COVID-19 pandemic situation or the conflict between the medical association and the government, may affect medical students’ internal learning environment. With the consecutive results of the learning environment, it is important to handle the external crises affecting the learning environment and improve each parts of the learning environment for medical students to focus more on their learning. Based on results of this study, further research is needed to analyze specific factors affecting the learning environment through student interviews.
Discussion
-
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Author contributions
All the work was done by SK.
Article information

Values are presented as mean±standard deviation or percentage of max.
DREEM, Dundee Ready Education Environment Measure; SPL, students’ perceptions of learning; SPT, students’ perceptions of teachers; SAS, students’ academic self-perceptions; SPA, students’ perceptions of atmosphere; SSS, students’ social self-perceptions.
DREEM, Dundee Ready Education Environment Measure; SS, sum of squares; df, degree of freedom; MS, mean square; SPL, students’ perceptions of learning; SPT, students’ perceptions of teachers; SAS, students’ academic self-perceptions; SPA, students’ perceptions of atmosphere; SSS, students’ social self-perceptions.
Values are presented as mean±standard deviation or percentage of max.
DREEM, Dundee Ready Education Environment Measure; SPL, students’ perceptions of learning; SPT, students’ perceptions of teachers; SAS, students’ academic self-perceptions; SPA, students’ perceptions of atmosphere; SSS, students’ social self-perceptions.
DREEM, Dundee Ready Education Environment Measure; SS, sum of squares; df, degree of freedom; MS, mean square; SPL, students’ perceptions of learning; SPT, students’ perceptions of teachers; SAS, students’ academic self-perceptions; SPA, students’ perceptions of atmosphere; SSS, students’ social self-perceptions.
Values are presented as mean±standard deviation or percentage of max.
DREEM, Dundee Ready Education Environment Measure; SPL, students’ perceptions of learning; SPT, students’ perceptions of teachers; SAS, students’ academic self-perceptions; SPA, students’ perceptions of atmosphere; SSS, students’ social self-perceptions.
DREEM, Dundee Ready Education Environment Measure; SS, sum of squares; df, degree of freedom; MS, mean square; SPL, students’ perceptions of learning; SPT, students’ perceptions of teachers; SAS, students’ academic self-perceptions; SPA, students’ perceptions of atmosphere; SSS, students’ social self-perceptions.
- 1. Skochelak SE, Stansfield RB, Dunham L, Dekhtyar M, Gruppen LD, Christianson C, et al. Medical student perceptions of the learning environment at the end of the first year: a 28-medical school collaborative. Acad Med 2016;91:1257–62.ArticlePubMed
- 2. Hutchinson L. Educational environment. BMJ 2003;326:810–2.ArticlePubMedPMC
- 3. Dyrbye LN, Thomas MR, Massie FS, Power DV, Eacker A, Harper W, et al. Burnout and suicidal ideation among U.S. medical students. Ann Intern Med 2008;149:334–41.ArticlePubMed
- 4. Audin K, Davy J, Barkham M. University Quality of Life and Learning (UNIQoLL): an approach to student well-being, satisfaction and institutional change. J Furth High Educ 2003;27:365–82.Article
- 5. Shochet RB, Colbert-Getz JM, Wright SM. The Johns Hopkins learning environment scale: measuring medical students' perceptions of the processes supporting professional formation. Acad Med 2015;90:810–8.ArticlePubMed
- 6. Jarvis-Selinger S, Pratt DD, Regehr G. Competency is not enough: integrating identity formation into the medical education discourse. Acad Med 2012;87:1185–90.ArticlePubMed
- 7. Cooke M, Irby DM, O’Brien BC. Educating physicians: a call for reform of medical school and residency. San Francisco: Jossey-Bass; 2010.
- 8. Chun K, Song Y. The achievement goal orientation differences of medical students according to the academic failure tolerance and self-efficacy. Korean J Educ Res 2011;49:183–211.
- 9. Kim SH, Jeon WT. The failure experiences of medical school students: a qualitative study. Korean J Med Educ 2008;20:351–62.Article
- 10. Jun SK, Park KH, Song PH, Bae YK, Kim SY. An exploratory study of factors affecting satisfaction of medical school life. Korean Med Educ Rev 2016;18:174–9.Article
- 11. Roff S, McAleer S, Harden RM, Al-Qahtani M, Ahmed AU, Deza H, et al. Development and validation of the Dundee Ready Education Environment Measure (DREEM). Med Teach 1997;19:295–9.Article
- 12. Roff S. The Dundee Ready Educational Environment Measure (DREEM): a generic instrument for measuring students' perceptions of undergraduate health professions curricula. Med Teach 2005;27:322–5.ArticlePubMed
- 13. Miles S, Swift L, Leinster SJ. The Dundee Ready Education Environment Measure (DREEM): a review of its adoption and use. Med Teach 2012;34:e620–34.ArticlePubMed
- 14. Park KH, Park JH, Kim S, Rhee JA, Kim JH, Ahn YJ, et al. Students' perception of the educational environment of medical schools in Korea: findings from a nationwide survey. Korean J Med Educ 2015;27:117–30.ArticlePubMedPMC
- 15. Yang EB, Meng KH. Five suggestions for future medical education in Korea. Korean J Med Educ 2014;26:167–78.ArticlePubMedPMC
- 16. Yu JH, Chae SJ, Chang KH. The relationship among self-efficacy, perfectionism and academic burnout in medical school students. Korean J Med Educ 2016;28:49–55.ArticlePubMedPMCPDF
- 17. Lee KH, Ko Y, Kang KH, Lee HK, Kang J, Hur Y. Mental health and coping strategies among medical students. Korean J Med Educ 2012;24:55–63.ArticlePubMedPMC
- 18. Kim B, Lee M, Kim K, Choi H, Lee SM. Longitudinal analysis of academic burnout in Korean middle school students. Stress Health 2015;31:281–9.ArticlePubMed
- 19. Chun KH, Park YS, Lee YH, Kim SY. Academic burnout and selection-optimization-compensation strategy in medical students. Korean J Med Educ 2014;26:299–308.ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite