An atypical case of Lemierre syndrome following oropharyngeal infection
Article information
Abstract
Lemierre syndrome is characterized by anaerobic bacterial infection in the head and neck and clinical or radiological evidence of internal jugular vein thrombophlebitis. The most common pathogens are Fusobacterium species, particularly Fusobacterium necrophorum. Septic emboli resulting from infected thrombophlebitis of the internal jugular vein leads to metastatic infections involving lung, liver, kidney, bone and central nervous system. The accurate diagnosis and treatment is important because it may be associated with a high mortality rate if untreated. We present a case of 28-year-old man with an atypical history for the diagnosis of Lemierre syndrome, which showed no definite evidence of internal jugular thrombophlebitis.
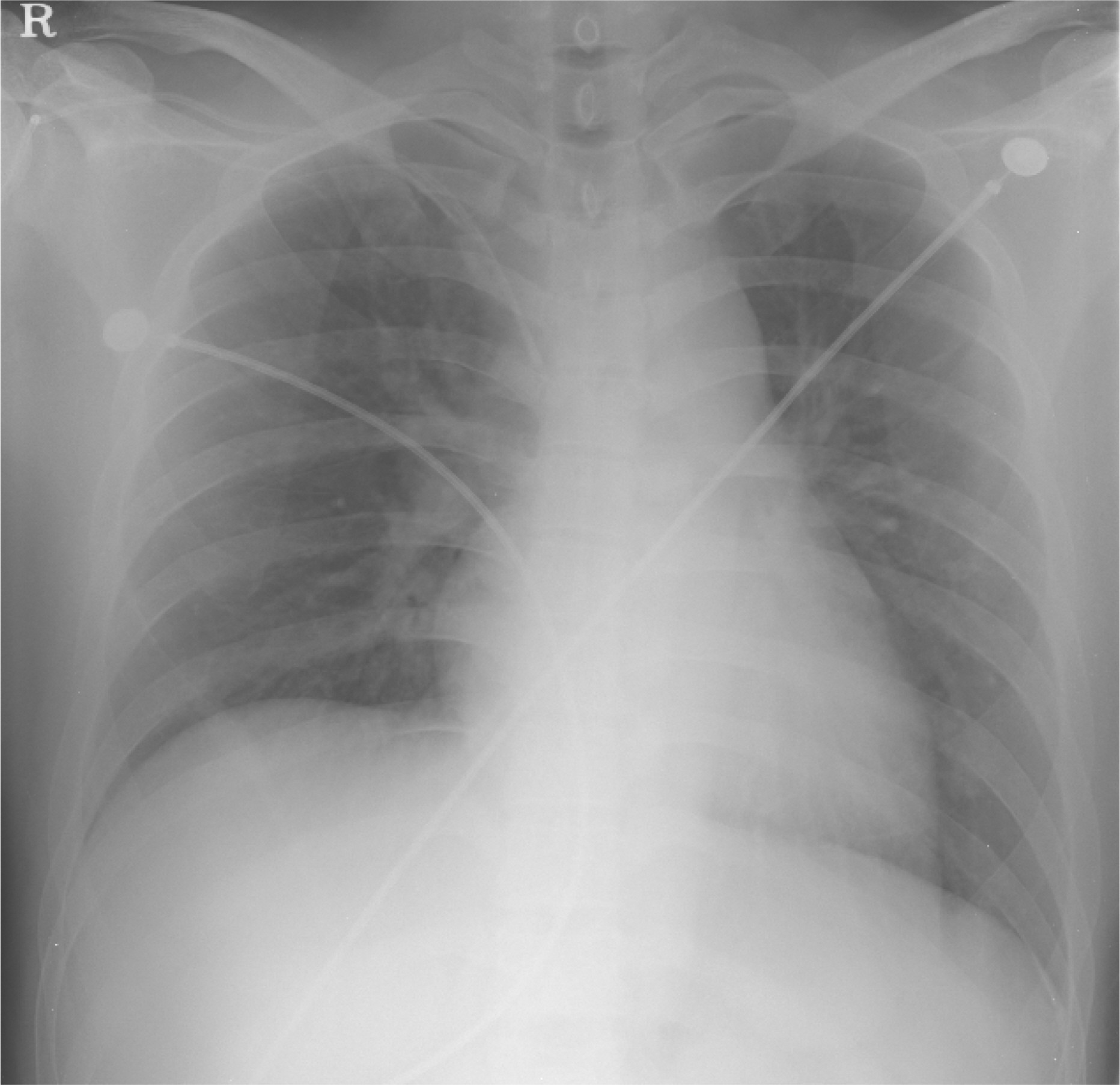
Chest X-ray (Admission day)
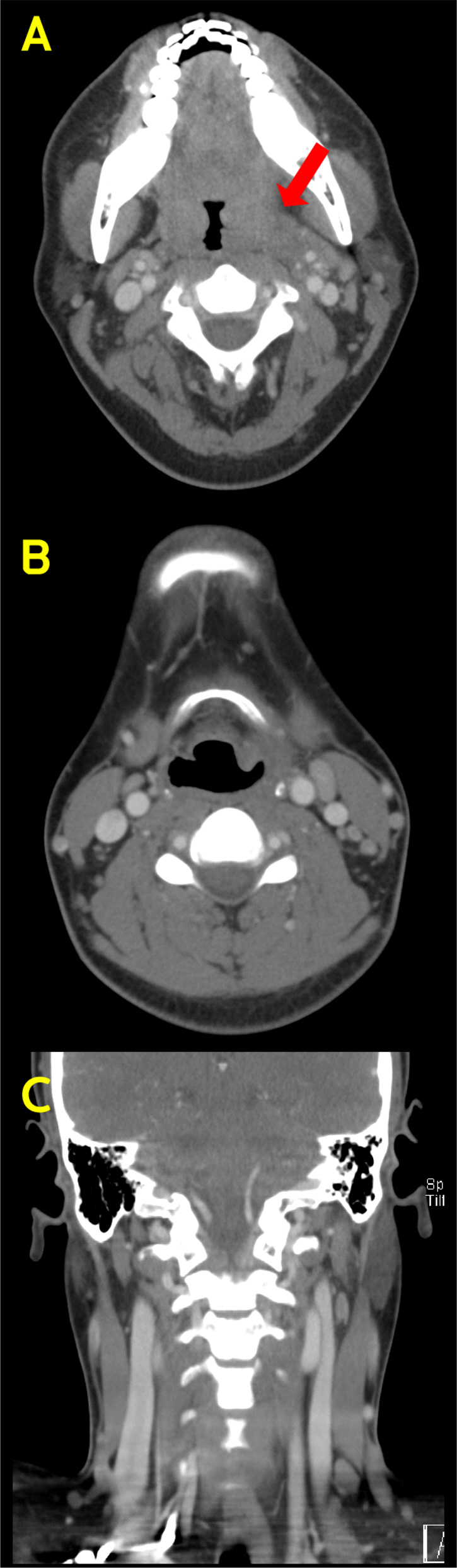
Computed tomography of neck. It shows diffuse enlargement of both tonsil (A) and reactive lymph nodes in both neck level II, III. (B) There is no definite evidence of internal jugular thrombophlebitis. (C)
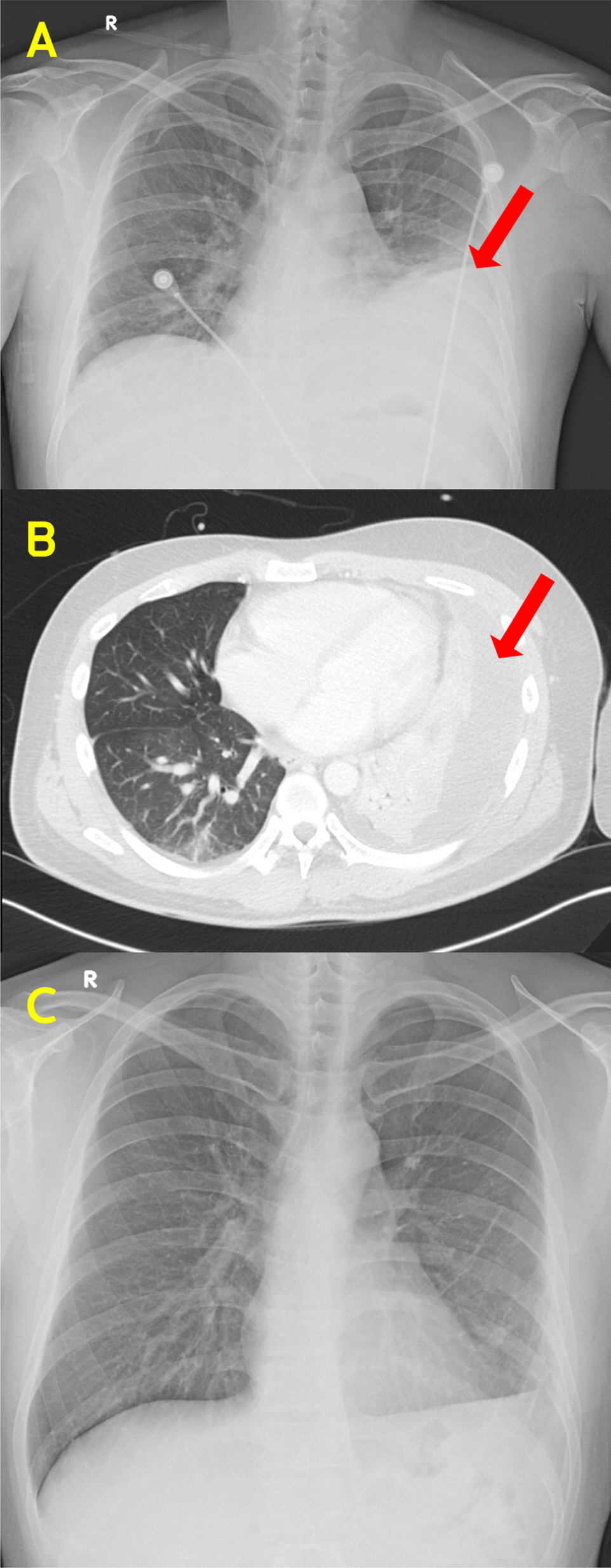
Chest X-ray and Computed tomography of chest. It shows empyema of left lung (arrow).