A 14-year-old boy with endobronchial carcinoid tumor presenting with asthma
Article information
Abstract
Introduction
Bronchial carcinoid tumors seldom occur in children, sometimes mistaken for a minor disease and diagnosed slowly. Materials and Methods: We report on a patient who diagnose tumors slowly because confused with asthma.
Results
This case describes a 14-year-old boy, presenting with asthma-like symptoms throughout 3 years. He was treated as asthma but wax and wane. Chest x-ray showed an hyperlucent left lung, so we rechecked high resolution computed tomography (HRCT) for unilateral hyperinflation diseases diagnosis. It was found 1×1㎝ nodule in left main bronchus. We did bronchoscopy and discovered a round mass in the left bronchus, 2∼3㎝ away from carina. In the biopsy, it was bronchial carcinoid tumor, so we resected tumor.
Discussion
Because symptoms of bronchial carcinoid tumors are various, it can often be misdiagnosed firstly. It is confused with asthma, pneumonia and foreign body. An additional examination were necessary when respiratory symptoms persist.
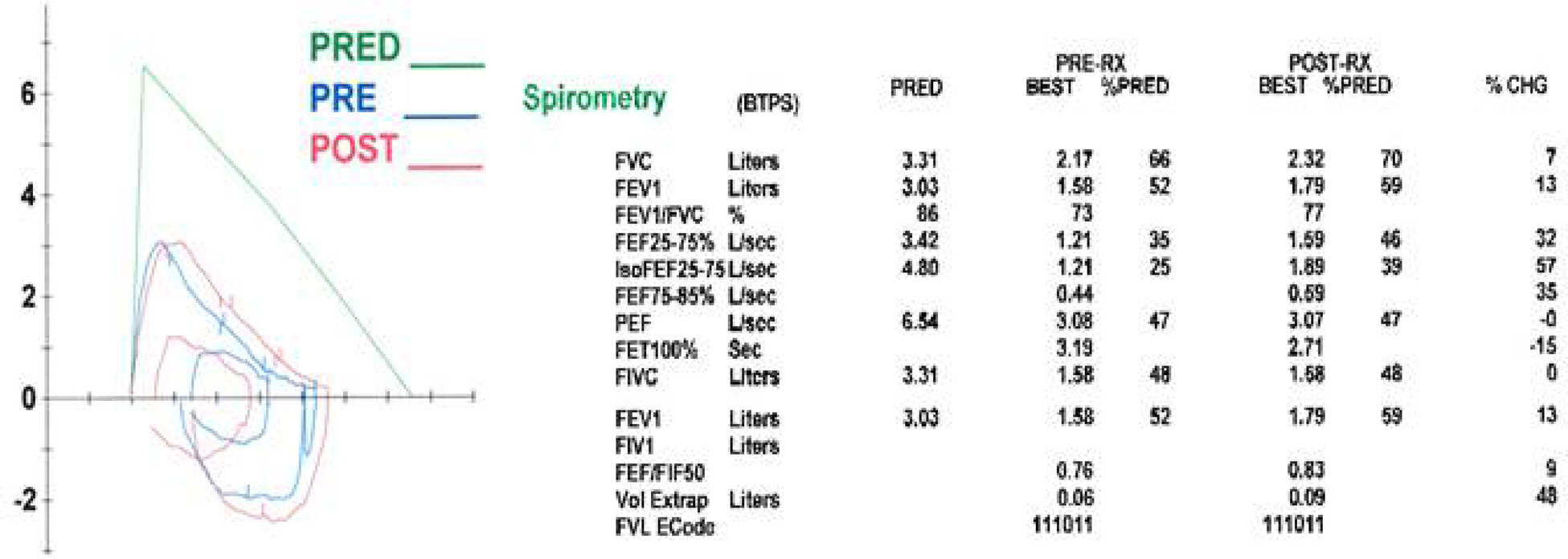
Spirometry shows obstructive lung disease with hypersensitivity of air way.

Chest x-ray shows both lung hyperinflation with Left lung hyperlucent lung field.

High resolution computed tomography (HRCT) shows an endobronchial nodule in Left main brohcus (1 x 1 cm).

Bronchoscopy before surgery shows a tumor obstructed left main bronchus from carina.

Bronchoscopy after surgery shows bronchus resected a tumor.