Peritoneal and gastric metastasis from invasive lobular breast carcinoma: a case report
Article information
Abstract
Abstract
Peritoneal and gastrointestinal metastasis from breast cancer is very rare. We report here a rare case of metastatic peritoneal and gastric cancer from breast lobular carcinoma after modified radical mastectomy. A 65-year old woman presented with anorexia, nausea, vomiting and dyspepsia for several weeks at 44 months after surgery. Radiologic study showed peritoneal metastasis, and surgical histopathology reported peritoneal and omental metastatic carcinoma. Esophagogastroduodenoscopic (EGD) biopsy also confirmed metastatic carcinoma originated from breast primary.
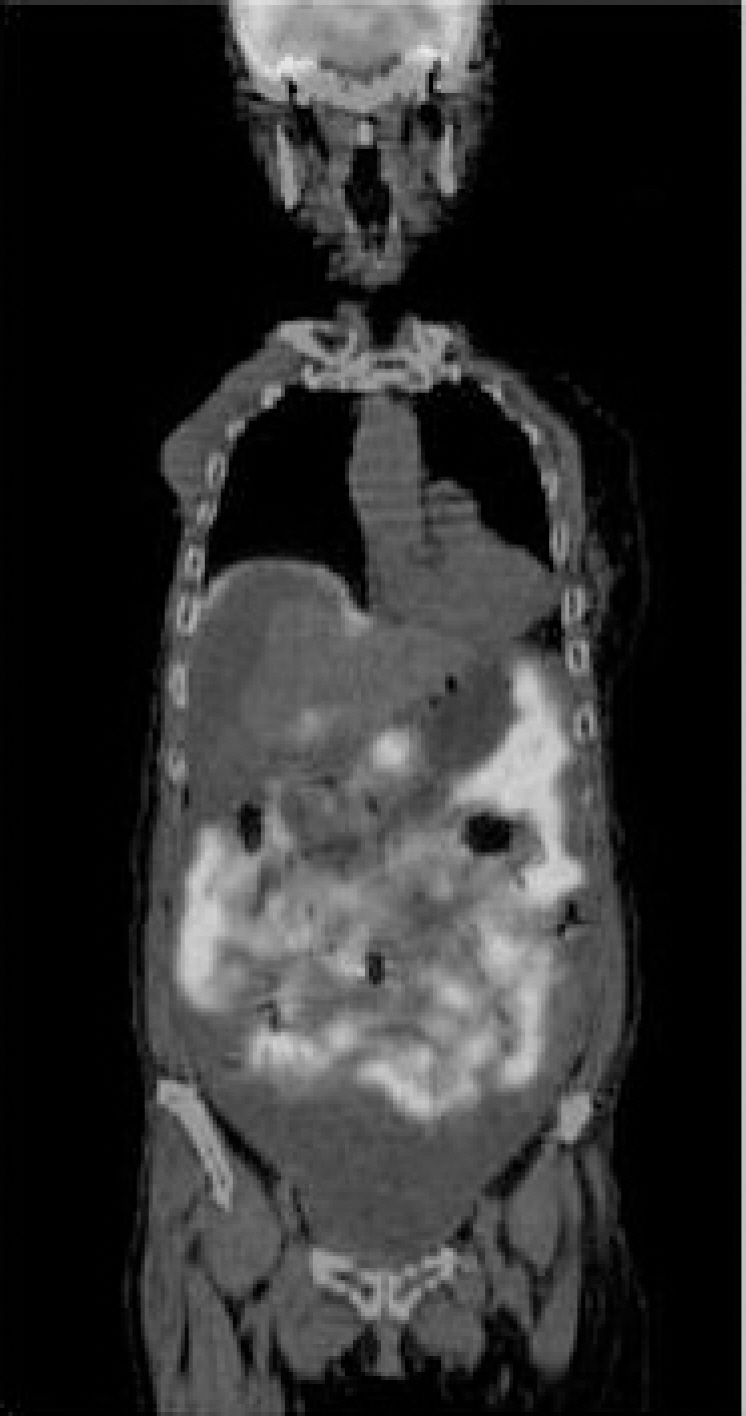
PET scan showed glucose hypermetabolism of abdominal cavity consistent with cancer peritonei. PET: positive emission tomography.

(A, B) Abdominal CT scans showed ascites, peritoneal thickening, omental smudge and cakes consistent with cancer peritonei. (C) Hydronephrotic change at the right kidney also presented. CT: computed tomography.
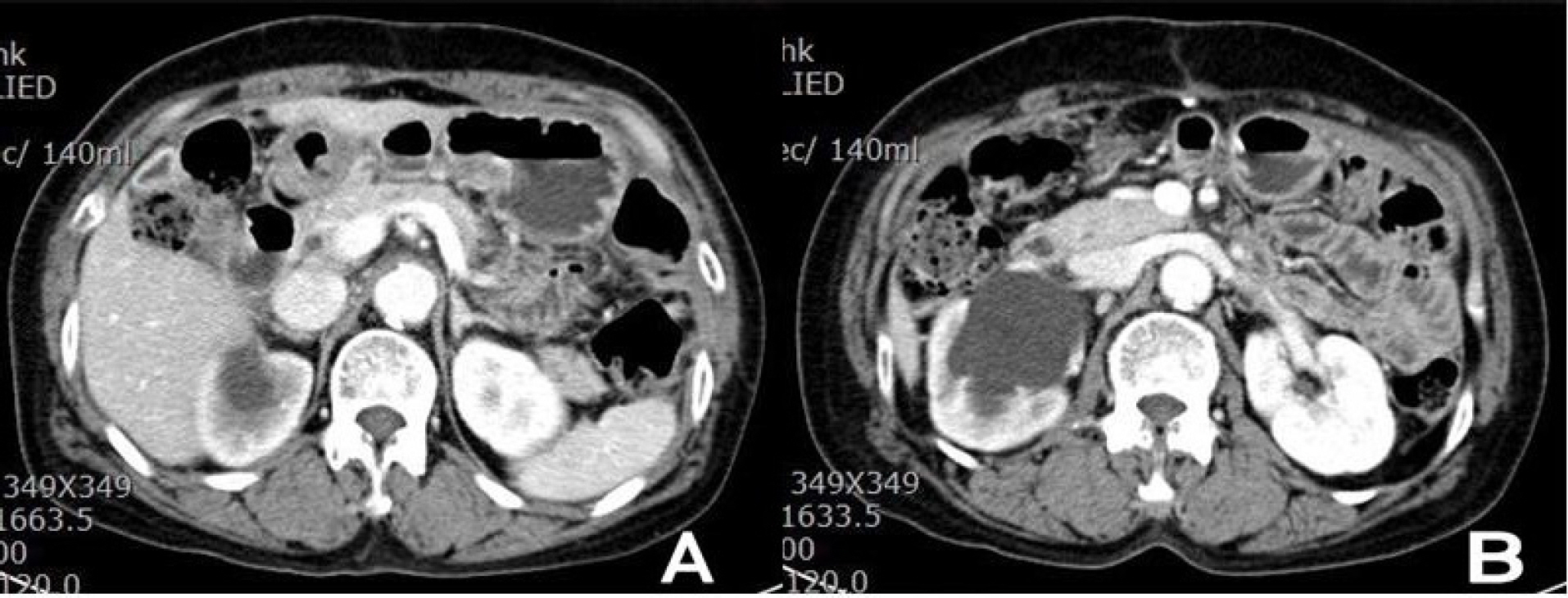
(A) After 9 cycles of chemotherapy, abdominal CT scans showed improving process with decreased ascites. (B) There are also hydronephrosis and hydroureter at the right kidney and ureter. CT: computed tomography.
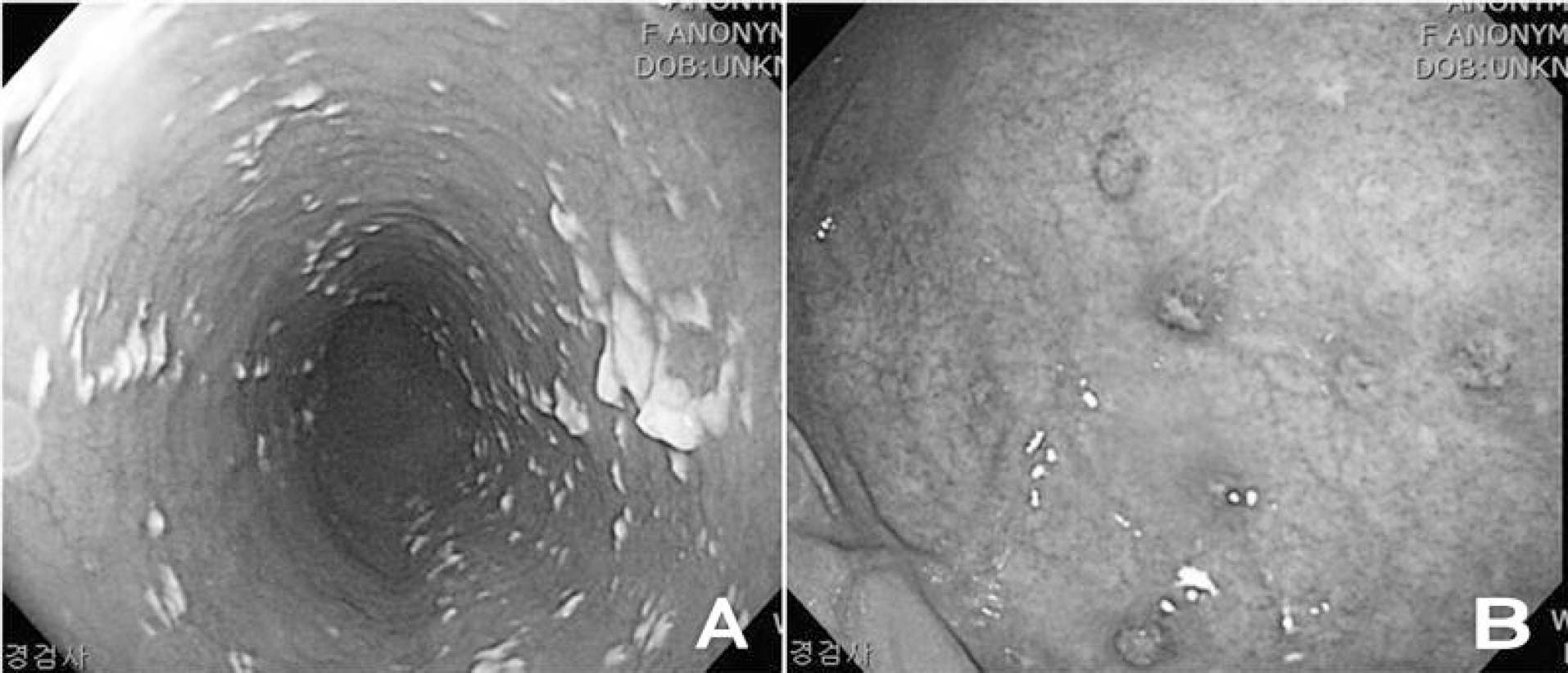
EGD showed (A) esophageal candidiasis at the esophagus and (B) metastatic gastric carcinoma from breast at the body of stomach. EGD: esophagogastroduodenoscopy.