Meningoencephalitis associated with Parvovirus B19 Infection in an Immunocompetent Patient
Article information
Abstract
Abstract
Parvovirus B19 (PVB19) infection is a rare cause of meningoencephalitis. A 53-year-old previously healthy woman presented with fever, headache, and multiple erythema on the both legs. Cerebrospinal fluid study revealed pleocytosis and elevated opening pressure and protein level. Brain MRI showed multiple, asymmetric, hyperintensity in the brain stem, basal ganglia, white matter, and gray matter. Anti-B19 IgM antibody and PCR for PVB19 were positive in serum. Clinician should consider PVB19 infection in any case of acute febrile illness with erythema and meningoencephalitis
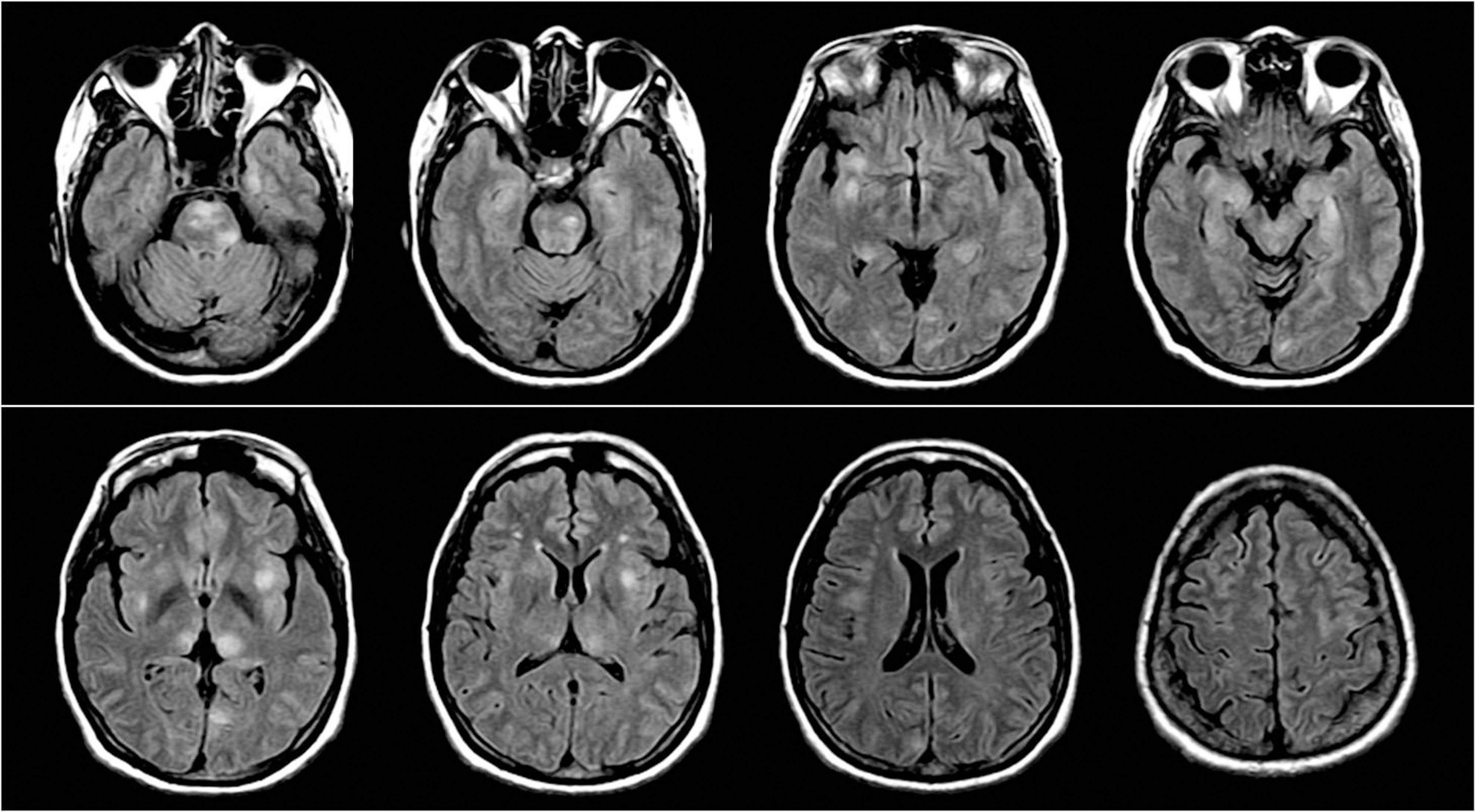
Axial FLAIR images show multiple, diffuse, asymmetric hyperintensities involving pons, midbrain, temporal lobe, bilateral thalami, basal ganglia, deep white matter, and temporal and occipital cortex.
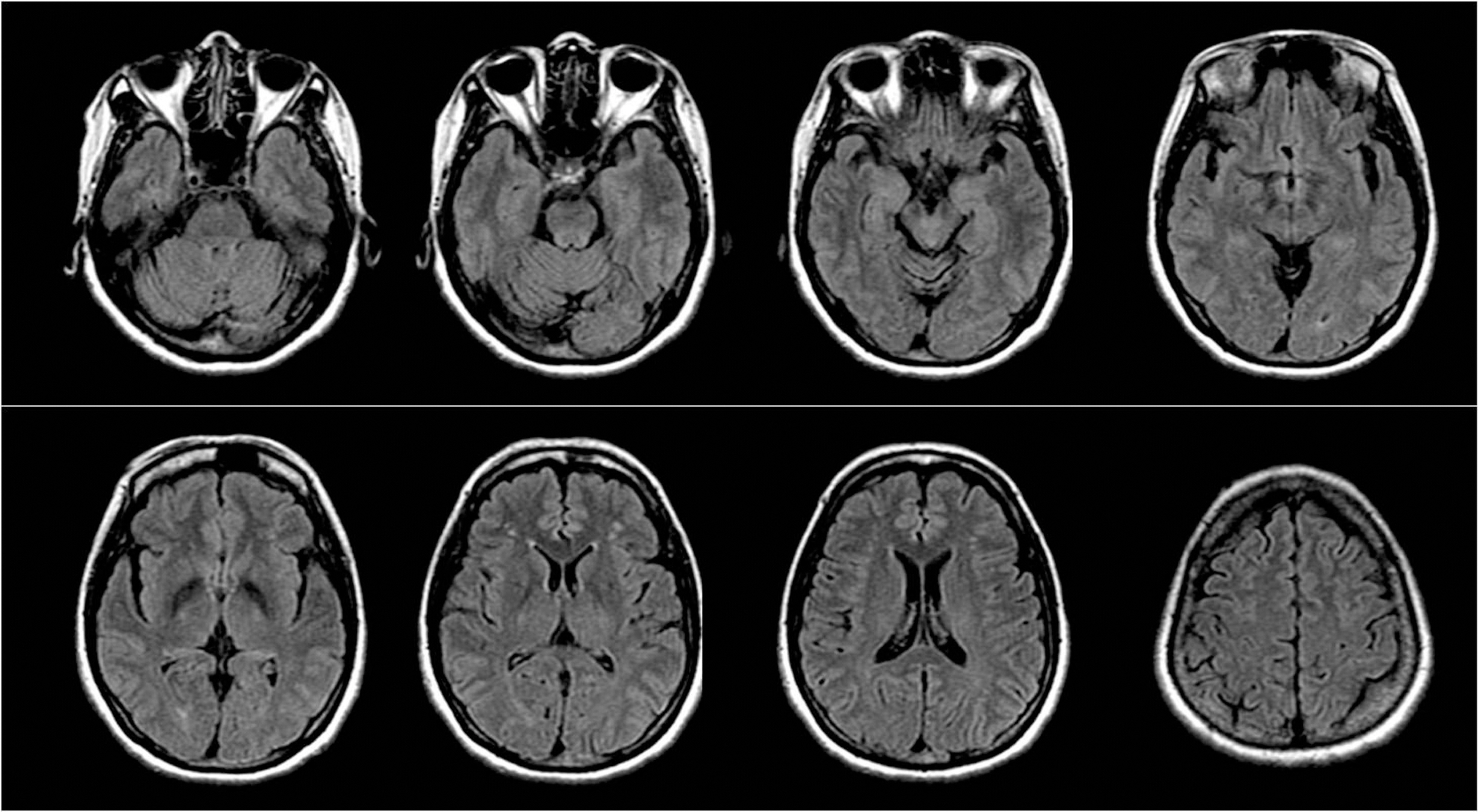
Follow-up FLAIR images 6 months later demonstrate normal without any residual lesions.