Post-traumatic tricuspid regurgitation with anterior papillary muscle rupture, corrected by papillary muscle reimplantation
Article information
Abstract
Abstract
A 60-year-old male patient with blunt chest trauma was transferred to our facility because of unstable vital signs and pericardial effusion. These conditions occurred after orthopedic surgery to repair multiple left finger fractures at a local medical center. Trans-thoracic echocardiography showed severe tricuspid regurgitation and he underwent papillary muscle reimplantation and tricuspid annuloplasty open heart surgery for post-traumatic tricuspid regurgitation with anterior papillary muscle rupture. We report early surgical traumatic valve disease correction without complications.

Chest computed tomography scan showed small amounts of pericardial effusion anterior to the right ventricle and right pleural effusion(A). Echocardiography showed that the tricuspid valve anterior leaflet had flailed papillary muscle(arrow)(B). Doppler echocardiography showed severe regurgitant flow at the right atrioventricular level during systole(C).
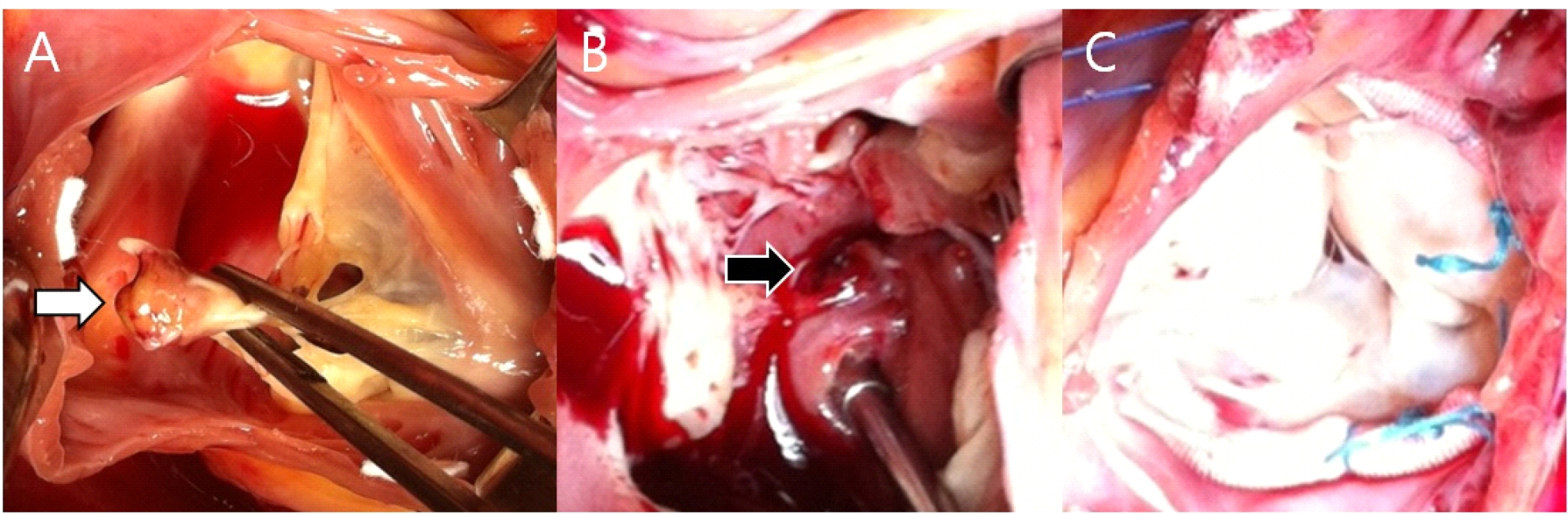
Intraoperative gross findings: Ruptured papillary muscle (PM) of the tricuspid valve anterior leaflet(arrow)(A), right ventricle ruptured PM stump(arrow)(B), and PM reimplantation and tricuspid annuloplasty with a 33mm Duranring(C).
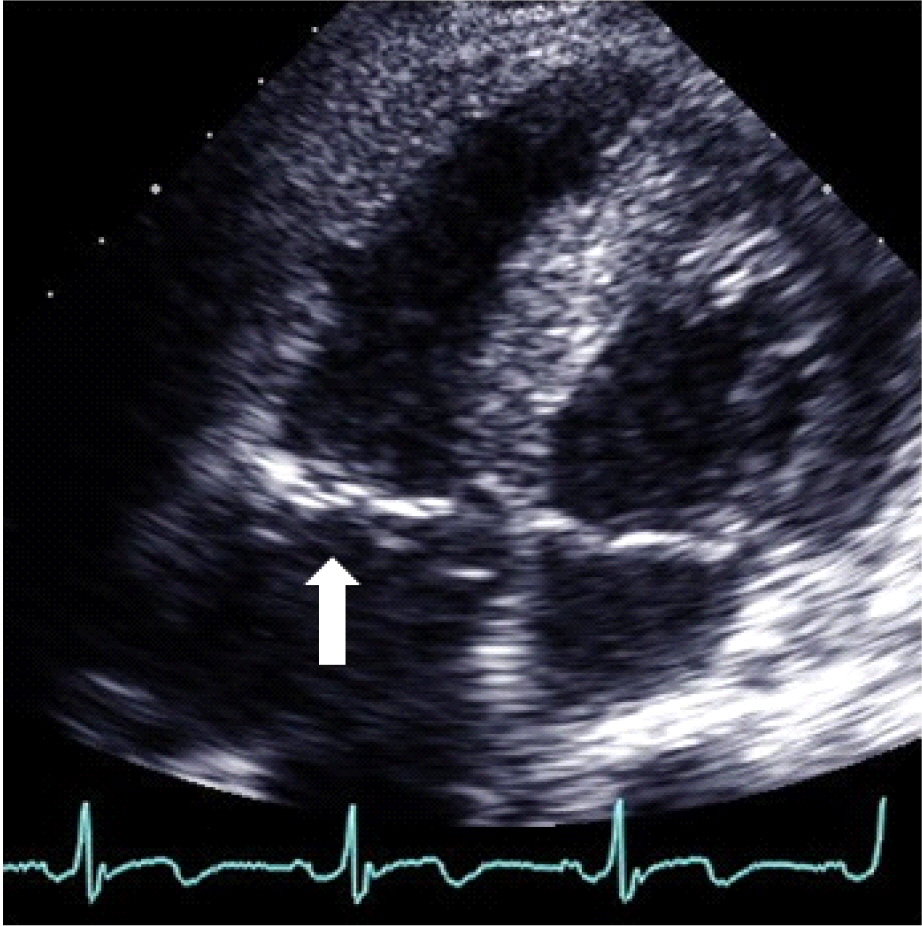
Echocardiography showed well coapted tricuspid valve leaflets(arrow) at the 7th postoperative day.