Laparoscopy-assisted Distal Gastrectomy with Systemic D2 Lymphadenectomy for Gastric Cancer: Usefulness of Noncompliance Rate to Validate the Completion of D2
Article information
Abstract
Objectives
Laparoscopy-assisted distal gastrectomy (LADG) is a common surgical procedure that has recently been accepted as safe and feasible for the treatment of early gastric cancer. There have been many efforts to expand the indications of LADG to include the treatment of advanced gastric cancer. The aim of this study was to determine the usefulness of noncompliance rate as an indicator for D2 lymph node dissection (LND) validation in LADG.
Methods
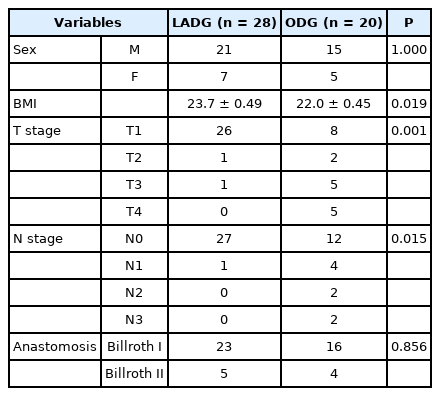
The subjects were 48 patients who underwent distal gastrectomy with D2 LND at Kosin University Gospel Hospital from October to December 2010. Of them, 28 underwent LADG and 20 underwent open distal gastrectomy (ODG). We compared several factors including noncompliance rate to validate D2 LND.
Results
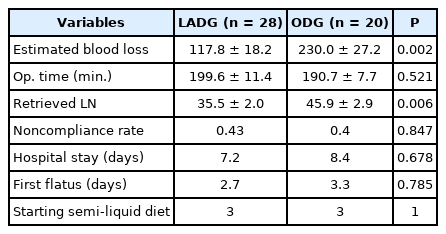
There were no significant differences in clinicopathologic factors except for BMI and tumor depth between the two groups. The average number of retrieved lymph nodes was significantly greater in the ODG group (45.9 ± 2.9) than in the LADG group (35.5 ± 2.0). The noncompliance rate was 43% in the LADG group and 40% in the ODG group with no significant difference.
Conclusions
In terms of no difference of noncompliance rate, LADG with D2 lymph node dissection is a safe, feasible and oncologicallycamparable with open gastrectomy. A large scaled prospective randomized trial should be needed to confirm the benefit of LADG.