A Case of Adrenal Tuberculosis with Atypical Clinical Manifestation
Article information
Abstract
Addison’s disease is a rare disorder that causes fatigue, genral weakness, weight loss, pigmentation due to adrenal hypofunction and it’s underlying causes are various. We report a case of 42-year-old man with fatigue, generalized cutaneous pigmentation. Computed tomography showed bilateral adrenal enlargement, but no calcification. Adrenal tuberculosis was established by ultrasound-guided fine needle aspiration biopsy.
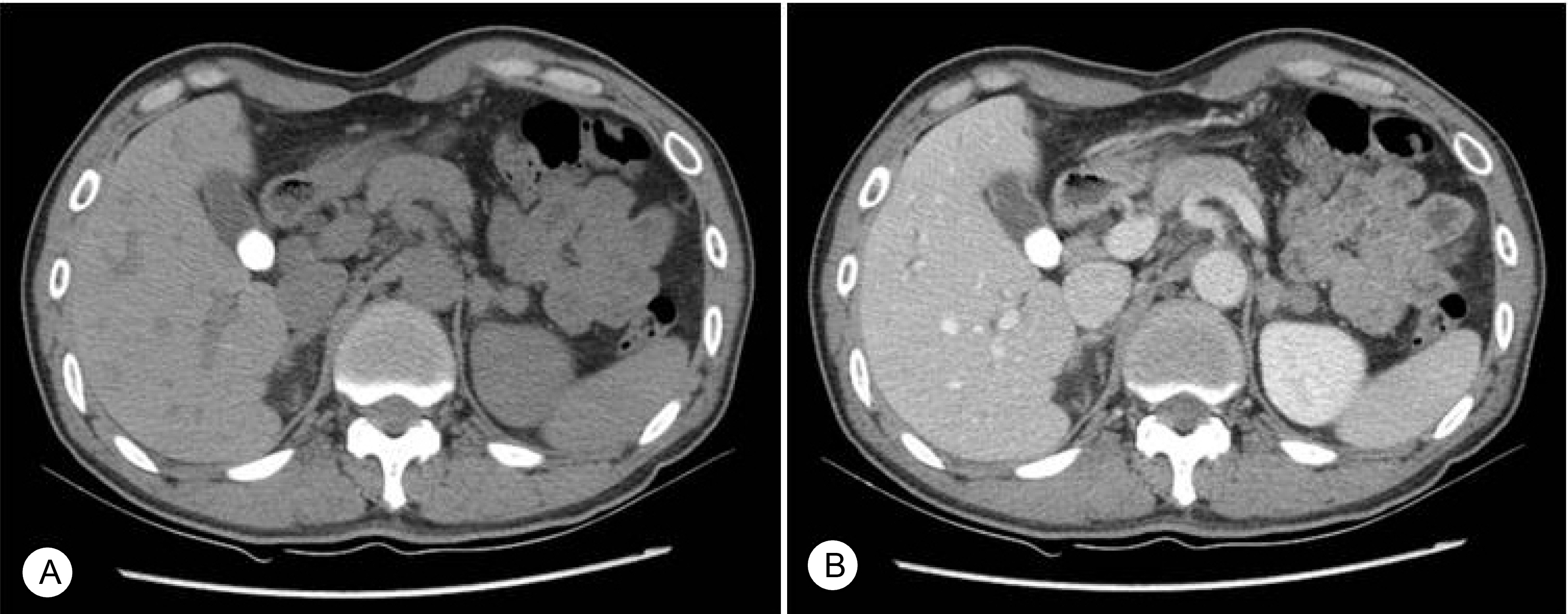
Dynamic adrenal gland computed tomography. Both adrenal gland show nodular hyperplasia and enlargement. (A) pre-enhance phase, (B) arterial phase.

Skin punch biopsy. The melanocytes are mildly increased in number (HE stain, × 400).

Adrenal gland, Fine needle aspiration biopsy. There is a caseation necrosis which is suspicious of tuberculosis (HE stain, × 400).