Dermoscopic features of an unusual case of targetoid hemosiderotic nevus
Article information

Abstract
Targetoid hemosiderotic nevus (THN) is a rare variant of melanocytic nevus, characterized by a sudden development of a targetoid ecchymotic halo around a pre-existing nevus. THN clinically raises concern for malignant transformation due to its abrupt change in color and size. THN should be distinguished from other diseases showing a peripheral halo, including targetoid hemosiderotic hemangioma, halo nevus, and Meyerson nevus. Dermoscopy can help clinicians to differentiate THN from these diseases. The typical dermoscopic features of THN are known to be divided into two distinctive areas: the central melanocytic area and the peripheral ecchymotic area. In our case, dermoscopy revealed a novel bull’s eye pattern composed of a central area with characteristic features of benign melanocytic nevus, an intermediated white circular ring, and a peripheral milky red area. When a sudden change occurs in a pre-existing nodule showing targetoid features, dermoscopy should be considered before conducting a biopsy or surgical intervention.
Introduction
Targetoid hemosiderotic nevus (THN), first described in 2005 by Tomasini et al. [1], is a variant of traumatized melanocytic nevus mimicking malignant melanoma. It needs to be evaluated carefully by a dermatologist to exclude the possibility of malignant transformation. Dermoscopy is a noninvasive method of diagnosis which allows the visualization of pigmented and vascular structures. It has been reported that dermoscopy reveals typical patterns of a benign melanocytic nevus on the central nodule in THN [1-3]. To date, there are only a few reports of dermoscopic features of THN. Herein, we report a case of THN with characteristic dermoscopic features.
Case
Ethical statements: This report was approved by the Institutional Review Board of Kosin University Gospel Hospital (IRB No. #2022-06-034). The patient in this manuscript has given written informed consent to the publication of his case details.
A 66-year-old man presented with a solitary, round, 2 cm in diameter, blackish nodule surrounded by an ecchymotic halo on the abdomen (Fig. 1). The lesion at first was a brownish nodule, which existed since birth. It had developed a sudden change in size and color within 3 days. The patient denied any type of overt trauma. He was not taking anticoagulant drugs at the time of the development of ecchymotic halo and did not complain any symptoms. Dermoscopic findings of the central nodule revealed brownish to violaceus globules intermingled with a structureless jet-black area. Dermoscopic findings of the peripheral ecchymotic halo revealed an intermediate white circular ring surrounded by a homogeneous milky red area (Fig. 2). Skin biopsy was performed with a suspicion of hemangioma or other melanocytic lesions, including melanoma. Histology of the completely excised nodule showed dome-shaped architecture, a well-circumscribed proliferation of melanocytes arranged in nests in the dermis, and extravasation of red blood cells throughout the lesion. Neither atypical cells nor mitoses were observed (Fig. 3). Based on clinicopathological findings, a diagnosis of THN was made. After 10 months of monitoring, there was no recurrence.

(A, B) Blackish nodule on the abdomen surrounded by an ecchymotic targetoid halo.

Dermoscopy revealed brownish globules (black arrows) and violaceus globules (white arrows) intermingled with a structureless jet-black area (white asterisk) on the center. On the periphery, homogeneous milky red areas (black arrowhead) with an intermediate whitish circular ring (black asterisk) surrounding the central nodule were seen (×10).
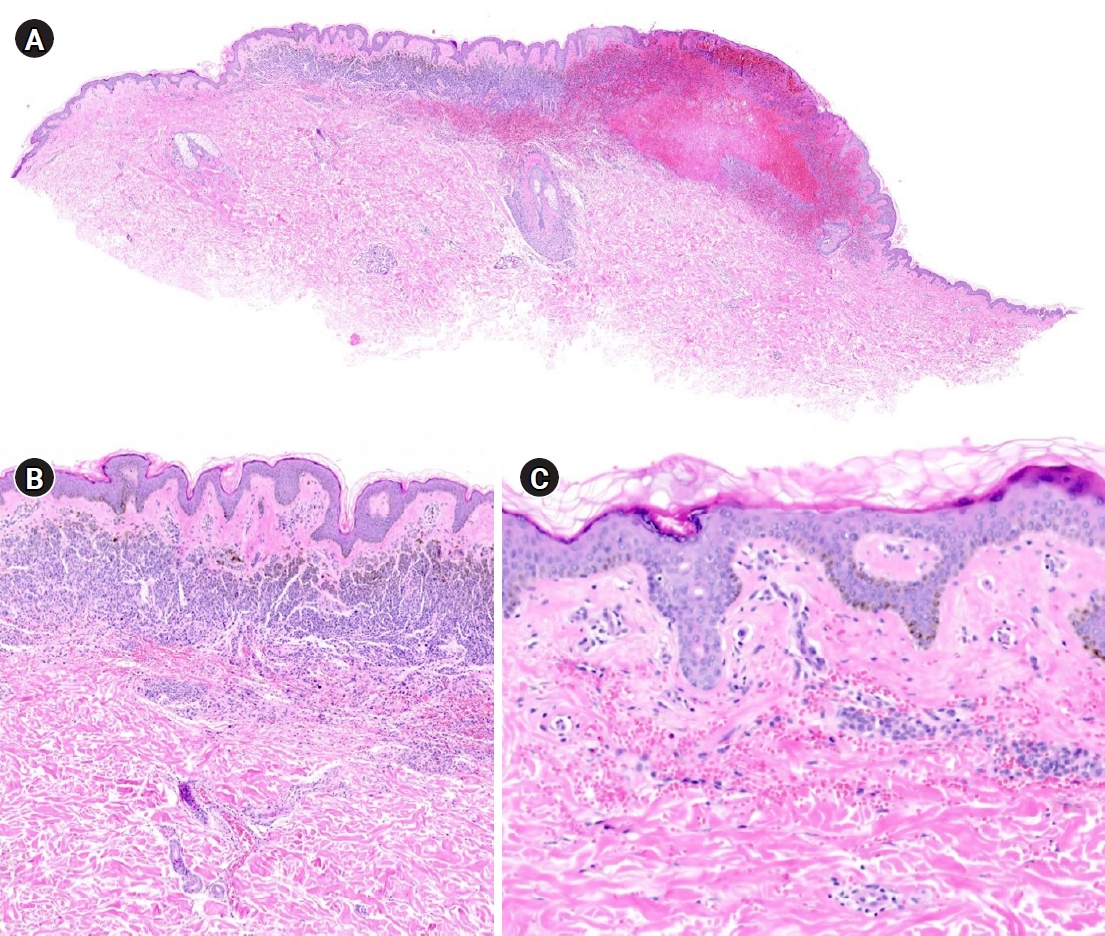
Histological findings. (A) Dome-shaped architecture was seen along with the extravasation of red blood cells throughout the lesion (hematoxylin-eosin [H&E] stain, ×20). (B) Well-circumscribed proliferation of dermal melanocytes arranged in a nest and vessel dilatation were noted (H&E stain, ×200). (C) On the periphery, only extravasation of red blood cells was seen (H&E stain, ×400).
Discussion
THN is a distinctive variant of traumatized melanocytic nevus. The pathomechanism of THN remains unclear, but it is presumed to be related to mild and repeated trauma. It has a predilection for the chest, abdomen, and shoulder, which are convex areas, and appears slightly elevated or exophytic, making it prone to receive chronic mechanical irritation. The peripheral ecchymotic halo usually appears abruptly without a history of overt trauma and regresses spontaneously within 4 weeks after the reabsorption of the extravasated red blood cells and hemosiderin with no recurrence [1,3]. Due to its benign nature, close observation using dermoscopy with short-term follow-up could be enough to manage it.
To date, it has been reported that dermoscopic findings of THN show two distinctive areas; benign melanocytic area on the center and homogeneous ecchymotic area on the periphery. Dermoscopy for the center shows a brownish globular pattern in addition to an irregular jet-black area and comma-shaped vessels. On the periphery, a homogeneous milky red area surrounding the entire lesion has been described [1-3]. Our case was novel in that an intermediate white circular ring was found between the central brown to black area and the peripheral homogenous milky red area, forming a bull’s eye pattern composed of three distinct zones.
THN should be distinguished from other diseases showing peripheral halo, including targetoid hemosiderotic hemangioma (THH), halo nevus, and Meyerson nevus. Dermoscopy can help clinicians to differentiate THN from these diseases.
The main differential diagnosis of THN is THH. On the naked eye examination, it is difficult to differentiate THH from THN because of their morphologic similarity; reddish to violaceous central nodule with the peripheral ecchymotic halo. On dermoscopy, THH presents as central red and/or dark lacunae characterized by multiple well-demarcated structures with a round to oval shape on the central nodule. An intermediate skin-colored, yellow, or whitish circular area surrounded by peripheral homogenous milky red area can also be found [4]. Our case of THN showed violaceus globules and an intermediate whitish circular area mimicking THH. However, the presence of brownish globules and structureless jet-black area, which are characteristic features of benign melanocytic nevus, made it possible to distinguish it from THH.
Halo nevus is characterized by a hypopigmented border around a pigmented melanocytic nevus. On dermoscopy, halo nevus has a peripheral rim of a whitish depigmented area rather than the peripheral reddish area found in THN [5]. Meyerson nevus is a benign melanocytic nevus with an eczematous halo. It is usually pruritic and presents with an erythematous scaly border. Meyerson nevus is dermoscopically differentiated from THN by the presence of yellow crusts, white scales, and dotted vessels [6].
In conclusion, dermoscopy considerably aids in the diagnosis of THN. In THN, dermoscopy reveals the bull’s eye pattern composed of three distinct zones, the central area with characteristic features of benign melanocytic nevus, the intermediated white circular ring, and the outermost homogenous milky red area. When a sudden change occurs in a pre-existing nodule showing targetoid features, dermoscopy should be considered first before conducting a biopsy or surgical intervention.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
None.
Author contributions
Conceptualization: MSJ. Data curation: JHJ. Formal analysis: DIK. Methodology: JYJ. Project administration: SHS. Visualization: JYJ. Writing - original draft: SMJ, JHJ. Writing - review & editing: SMJ, JBP, MSJ. Approval of final manuscript: all authors.