Effectiveness of prophylactic calcium and vitamin D supplementation for preventing post-thyroidectomy hypocalcemia: a meta-analysis
Article information

Abstract
Background
Postsurgical hypocalcemia is the most common and troublesome consequence of thyroidectomy. We investigated the potential role of routine calcium or vitamin D supplementation in preventing postsurgical hypocalcemia.
Methods
We searched MEDLINE and Embase for English-language publications using the keywords “calcium,” “vitamin D,” and “thyroid cancer.” The primary outcome was any postoperative hypocalcemia, and the secondary outcome was symptomatic hypocalcemia.
Results
Four studies that included 381 patients were eligible for this meta-analysis. A random-effects model showed no significant difference in the occurrence of hypocalcemia between calcium/vitamin D treatment and placebo/no treatment. However, the occurrence of symptomatic hypocalcemia was lower in patients with calcium/vitamin D treatment. In the combined results, preoperative calcium and vitamin D supplementation were associated with a reduced incidence of symptomatic hypocalcemia.
Conclusions
Our findings support the use of preoperative calcium and vitamin D supplementation in conjunction with routine postsurgical supplementation for patients after total thyroidectomy.
Introduction
Thyroid cancer is the most common type of malignant endocrine cancer, and its incidence is continuing to rise worldwide [1]. Total thyroidectomy followed by radioactive iodine treatment together with life-long administration of thyroid hormone is the treatment strategy for most patients with thyroid cancer [2]. Total thyroidectomy is one of the most common endocrine-gland operations and most patients recover fully without any adverse events [3]. Hypoparathyroidism (hypoPTH) and hypocalcemia are the most common and troublesome long-term consequence of bilateral and reoperative thyroid operations [4,5]. Large epidemiologic studies have estimated that the overall incidence of hypoPTH after anterior neck surgery is approximately 8%, with 75% of cases resolving within 6 months and the remaining 25% resulting in permanent hypoPTH [6]. Postsurgical hypocalcemia impacts negatively of patient’s quality of life due to the need for lifetime medication, regular visits and significant long-term costs. Most transient hypocalcemias may not warrant long‑term calcium and vitamin D supplementation [3]. The most common early symptoms of postsurgical hypocalcemia are paresthesias, or numbness and tingling, of the perioral region and the fingertips. More sustained muscle contraction may lead to laryngospasm, and more severe neural excitability may lead to seizures. Moreover, severe hypocalcemia can cause life-threatening complications, such as laryngospasm and cardiac arrhythmias [4,7]. Therefore, close monitoring of calcium and parathyroid hormone (PTH) levels is indicated in order to identify hypoPTH before the development of severe, symptomatic hypocalcemia after surgery [6].
An empirical prophylactic approach for managing potential post-thyroidectomy hypocalcemia is to prescribe oral calcium routinely with or without oral calcitriol, without testing PTH or calcium levels [8,9]. This approach is cost-effective, is not labor intensive, is expeditious, and can hasten hospital discharge after thyroidectomy [4]. Previous studies have shown the efficacy of routine postsurgical calcium and vitamin D supplementation as a prophylactic strategy to prevent hypocalcemia in patients undergoing total thyroidectomy [10-12], but the effectiveness of preoperative supplementation is limited. Moreover, there is no consensus on the role of routine calcium and/or vitamin D before thyroid surgery [11].
Our objectives in this meta-analysis are to evaluate the potential role of routine calcium and vitamin D supplementation for the prevention of postsurgical hypocalcemia and to draw therapy guidelines that may prevent this common complication.
Methods
1. Data search and study selection
We did a systematic search for studies from MEDLINE (inception to March 2019) and Embase (inception to March 2019) using the keywords “calcium” and “thyroid cancer” or “vitamin D” and “thyroid cancer.” The primary analysis included studies comparing the occurrence of postsurgical hypocalcemia in subjects with thyroid cancer who had preoperative calcium or vitamin D treatment. Manual searches included scanning of reference lists for relevant studies and eligible articles. We included articles written in English only in this study. Two of us conducted the search of our own, and disagreements were settled by discussion.
2. Data extraction
We extracted data from the publications and recorded the following information independently: first author, year of publication, country, data source, the number of patients and centers enrolled in the study, dosage of calcium or vitamin D, and definition of hypocalcemia. For the outcome data, we calculated the odds ratios (ORs) from the number of cases in which hypocalcemia occurred in each group.
3. Statistical analysis
The primary outcome was any postoperative hypocalcemia, and the secondary outcome was symptomatic hypocalcemia. We analyzed data from each study using Review Manager (RevMan, version 5.2, Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012). We reported outcome measures as ORs and 95% confidence intervals (CIs), using a fixed-effect or random-effects model according to Mantel and Haenszel, and presented the results as forest plots. An OR greater than 1 implied more hypocalcemia for preoperative calcium or vitamin D users, whereas an OR less than 1 implied less hypocalcemia for such users. Heterogeneity of the studies were assessed using the chi-square test of heterogeneity; I2 >50% was considered significant heterogeneity, as described by Higgins et al. [13]. A p<0.05 was considered to indicate statistical significance.
Results
1. Study characteristics
We identified 607 articles through the database. After excluding conference abstracts (n=135), non-human studies (n=108), and non-English studies (n=49), we assessed 315 abstracts for eligibility. After reviewing full-text articles, four studies that included 381 patients were eligible for this analysis [14-17]. The details of the study selection process are depicted as a flowchart (Fig. 1). The summary of studies included is presented in Table 1.

Flowchart.

Study characteristics
2. Hypocalcemia
1) Any postoperative hypocalcemia
Three studies covering 306 patients among four studies were included in analyzing postoperative hypocalcemia. The random-effects model showed no significant difference in the occurrence of hypocalcemia between calcium/vitamin D treatment and placebo/no treatment (OR, 0.82; 95% CI, 0.36–1.86; I2=60%, p=0.63) (Fig. 2).
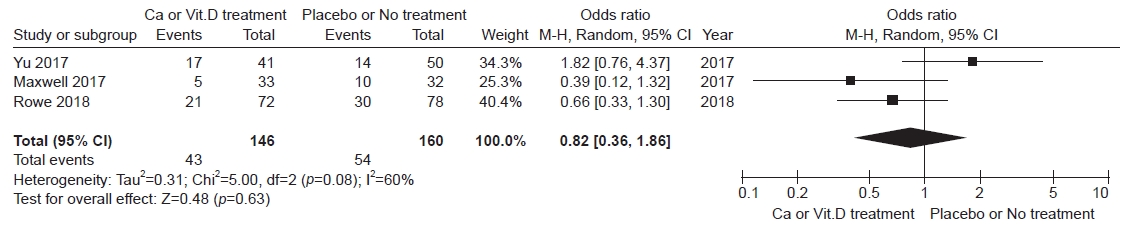
Forest plot of any postoperative hypocalcemia. Ca, calcium; Vit.D, vitamin D; CI, confidence interval; M-H, Mantel and Haenszel.
2) Symptomatic hypocalcemia
Three studies covering 275 patients among four studies were included in analyzing postoperative hypocalcemia. The occurrence of symptomatic hypocalcemia was lower in patients with calcium/vitamin D treatment than in those with placebo/no treatment (OR, 0.44; 95% CI, 0.22–0.88; I2=41%, p=0.02) (Fig. 3).
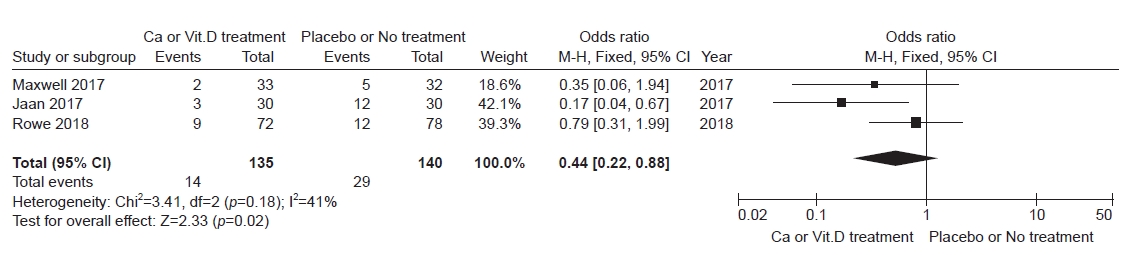
Forest plot of symptomatic hypocalcemia. Ca, calcium; Vit.D, vitamin D; CI, confidence interval; M-H, Mantel and Haenszel.
Discussion
The mainstay of therapy for differentiated thyroid cancer is thyroidectomy [2]. Postsurgical hypocalcemia following thyroidectomy is a common complication because of damage to the parathyroid glands. It also increases healthcare‐associated expenditure because of increased monitoring requirements, pharmacotherapy, and prolonged hospitalization in addition to patient morbidity, Interventions that minimize postsurgical hypocalcemia are needed in order to improve patient care and waste of resources. In combined results, we found that preoperative calcium and vitamin D supplementation was associated with a reduced incidence of symptomatic hypocalcemia after total thyroidectomy.
The mechanisms of postsurgical hypoPTH are related to disruption of parathyroid arterial supply or venous drainage, mechanical, thermal or electrical injury, and partial or complete removal [18]. Therefore, the most straightforward way to avoid hypoPTH is to limit the extent of thyroidectomy to a unilateral approach [4]. The best prophylaxis to avoid postsurgical hypocalcemia after total thyroidectomy is parathyroid gland preservation during operation to preserve the blood supply to the parathyroid glands [19]. Even when these glands are thought to be well preserved during surgery, normal postsurgical parathyroid function is not guaranteed [20].
Several interventions to reduce the incidence of postsurgical hypocalcemia have been suggested because patients with symptomatic hypocalcemia undergoes physical and mental suffering [12]. Therefore, routine calcium and vitamin D supplementation is advocated in many clinical centers [4,19]. These prophylactic approaches to prevent postsurgical hypocalcemia is to routine prescription of oral calcium with or without calcitriol [8,9]. Typically, oral calcium carbonate is the most widely available and inexpensive preparation and is given as 500–625 mg to 1,000–1,250 mg two to three times a day. This routine administration of oral calcium is known to reduce postsurgical hypocalcemia to approximately 10% [21]. Because of low cost and ease of dosing for patients at risk for hypoPTH, we also recommend universal calcium prophylaxis like others [19].
Vitamin D deficiency is an independent risk factor of postsurgical hypocalcemia [5]. Moreover, the severity of hypocalcemia seems to be remarkably higher in those with lower than normal preoperative vitamin D levels [22,23]. Therefore, prophylactic treatment of hypocalcemia with vitamin D and calcium is a reasonable strategy with synergy [24]. Impaired PTH secretion with inhibition of bone resorption, reduction of vitamin D synthesis by the kidneys, and reduced intestinal absorption of calcium results in postoperative hypocalcemia [25]. Adding calcitriol (1,25-(OH)2-D3) adds to the cost but increases the effectiveness of oral calcium. It also increases calcium absorption and increasing intestinal calcium transport into the blood. This effect on calcium absorption usually takes few days [14]. Therefore, preoperative supplementation in patients undergoing thyroidectomy with calcitriol are expected to increase the efficacy of routine calcium supplementation in the immediate postsurgical period, thereby decreasing the duration of transient hypocalcemia [4].
PTH level has also been suggested as a reliable marker of postsurgical permanent hypoPTH [26]. However, development of acute hypocalcemia after thyroid surgery lags behind the decline in the serum PTH level, and the patient may have been from the hospital before their serum calcium having reaches a nadir, which may occur 24 to 72 hours after thyroidectomy [4]. Therefore, it is important to anticipate the possibility of progressive hypocalcemia, to educate patients about its possible development and steps they should take to avoid and treat it, and to institute preemptive measures that both prevent and correct hypocalcemia in the presurgical period.
Postoperative calcium plus vitamin D is known to be effective in preventing postoperative hypocalcemia and decreasing the demand for intravenous calcium supplementation [12]. This meta-analysis found the role of preoperative oral calcium and vitamin D supplementation in avoiding postsurgical symptomatic hypocalcemia. This prophylactic approach may cause uncommon but serious risks of overshooting and causing hypercalcemia and potential renal injury. Therefore, biochemical monitoring for medication tapering is mandatory [4]. However, the half-life of calcitriol is relatively short (5–8 hours), and toxicity from excessive calcitriol ingestion may be reversed quickly (within days) [4].
Our study has some limitations. First, the studies included in the meta-analysis were heterogeneous. There was a high heterogeneity especially among the studies including those at a young age. There is no universal agreement on standardized definitions for postsurgical hypocalcemia and hypoPTH after total thyroidectomy [11]. The reported incidence of postsurgical hypoPTH varies differs greatly, and previous research also suggested that the definition of hypoPTH is not universal throughout the literature [11]. Second, attempting to compare data from the surgical series is difficult and may be inaccurate. Analysis was even more difficult by the diversity of postsurgical electrolyte supplementation protocols used by different doctors. Third, we cannot define the adequate dosage and duration of calcium and vitamin D intake before surgery, because the regimens of each study studies were quite variable very different. Lastly, small numbers of studies included in this meta-analysis might be exposed to publication bias.
Postsurgical hypocalcemia is the most common complication of total thyroidectomy. Increased recognition and early implementation of various strategies can improve clinical outcomes and quality of life. We support the use of preoperative calcium and vitamin D supplementation in conjunction with routine postsurgical supplementation for patients after total thyroidectomy.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Funding
This work was supported by the research fund of Dong-A University.
Author contributions
Conceptualization: KP, SS. Data curation: JWS, KK, IJK, KP. Formal analysis: KK, KP. Investigation: HM, HYK, MKP, KP, SS. Methodology: KP, SS. Visualization: KK, KP, SS. Writing - review & editing: HM, HYK, MKP, KP, SS. Approval of final manuscript: all authors.