Clinical Features and Histological Findings of 17 Patients with Chronic Actinic Dermatitis
Article information
Abstract
Objectives
This study was designed to evaluate the clinical, histological and immunohistochemical findings and treatment of chronic actinic dermatitis in Korean patients.
Methods
Seventeen Korean patients with chronic actinic dermatitis were enrolled for this study. The clinical and histological findings and the results of phototest were reviewed with medical records, clinical photographs and pathologic slides. We also reviewed the effectiveness of the treatments in all patients with chronic actinic dermatitis.
Results
In all patients with chronic actinic dermatitis, pruritus was severe, and the patients present in the early stages with erythemas on the face, neck and the back of the hands. As the eruption progresses, it became lichenified and scaly plaques and papules developed. The face, upper extremity and neck were most commonly affected. The most common abnormal results of the phototests were decreased MED-UVB alone. In 8 patients with actinic reticuloid, histopathologic findings showed irregular acanthosis, parakeratosis, spongiosis, atypical hyperchromatic cells with cerebriform nuclei, epidermotropism, Pautrier-like microabscess, deep perivascular lymphocytic infiltrates, vertically-streaked collagen in the papillary dermis, stellate and multinucleated fibroblasts. Treatment includes topical tacrolimus and corticosteroid, oral corticosteroid, azathioprine and cyclosporine.
Conclusions
Our study showed classic clinical and histological findings. The most common abnormal results of the phototests were decreased MED-UVB alone. Topical steroid, tacrolimus and systemic cyclosporine, azathioprine are effective in treating chronic actinic dermatitis.
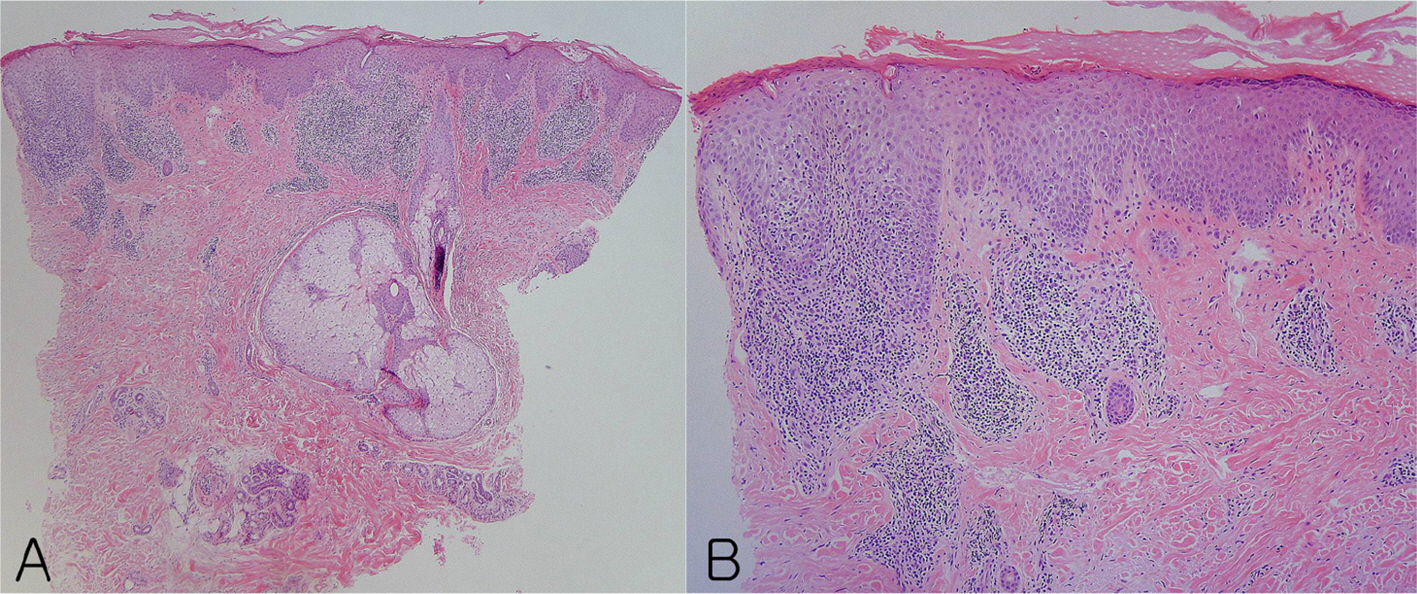
(A) Irregular acanthosis, and lymphocytic infiltration in the papillary dermis and reticular dermis (H&E, x 40), (B) Epidermotropism, irregular acanthosis and a perivascular infiltrate of the papillary dermis (H&E, x 100) (Case 16).
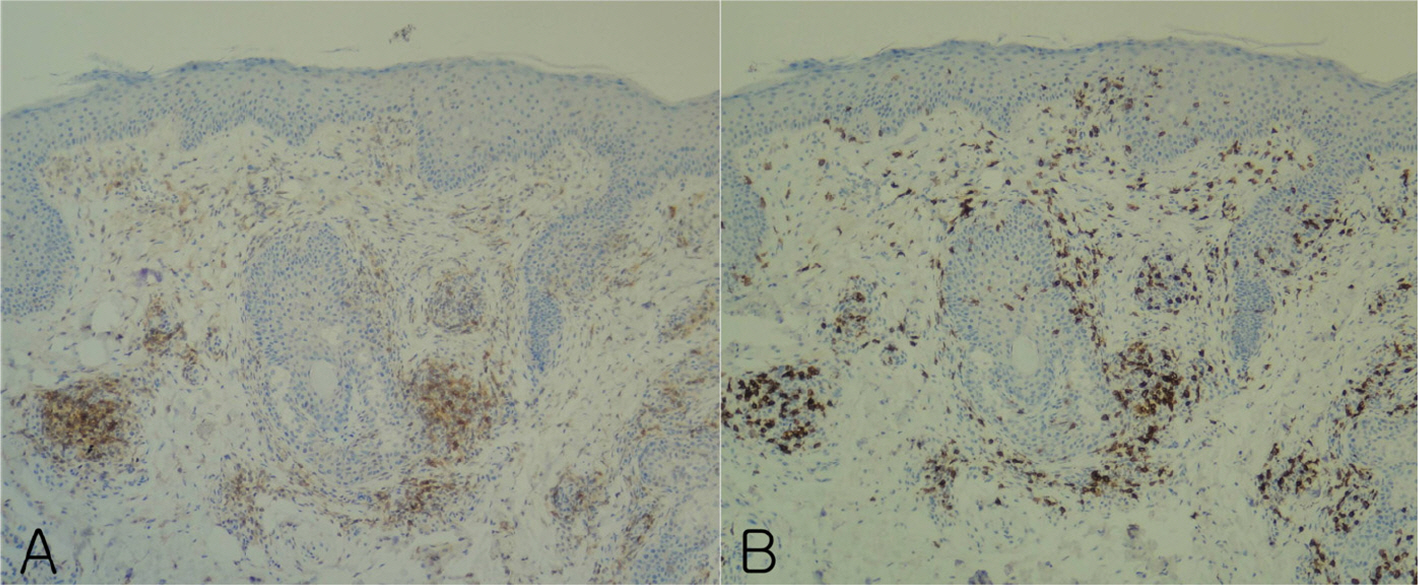
Immunohistochemical studies showed that CD4 positive T cells (A) and CD8 positive T cells (B) were in the epidermis and dermis (x 100). CD8 positive T cells predominated in the epidermis (B) compared to CD4 positive T cells (A). (Case 6).

Immunohistochemical studies showed that CD4 positive T cells (A) and CD8 positive T cells (B) were in the epidermis and dermis (x 100). CD8 positive T cells predominated in the epidermis (B) compared to CD4 positive T cells (A). (Case 6).

Immunohistochemical studies showed that CD4 positive T cells (A) and CD8 positive T cells (B) were in the epidermis and dermis (x 100). CD8 positive T cells predominated in the epidermis (B) compared to CD4 positive T cells (A). (Case 6).

Summary of clinical characteristics in patients with chronic actinic dermatitis

Results of phototests in patients with chronic actinic dermatitis

Results of photopatch tests in patients with chronic actinic dermatitis

Summary of treatment in patients with chronic actinic dermatitis