KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 32(1); 2017 > Article
-
Case Report
Kearns-sayre Syndrome Treated with Permanent Pacemaker Insertion for Complete Atrioventricular Block - Eun Hye Park, Sung Ho Her, Myung A Ha, Hyo Suk Kim, Jae Hyuk Jang
-
Kosin Medical Journal 2017;32(1):133-138.
DOI: https://doi.org/10.7180/kmj.2017.32.1.133
Published online: June 30, 2017
Division of Cardiology, College of Medicine, the Catholic University of Korea, Seoul, Korea.
- Corresponding Author: Sung Ho Her, Daejeon St. Mary's hospital, 642 Daeheung-ro, Jung-gu, Daejeon 34943, Korea. Tel: +82-042-220-9504, Fax: +82-042-226-9686, hhhsungho@naver.com
• Received: May 13, 2016 • Revised: July 7, 2016 • Accepted: July 25, 2016
Copyright © 2016 Kosin University College of Medicine
- 960 Views
- 3 Download
Abstract
- Kearns-Sayre syndrome (KSS) is a rare multisystem mitochondrial disorder associated with progressive external ophthalmoplegia, atypical pigmentary degeneration of the retina, and complete heart block. KSS can lead to a risk of sudden death because of the potential progression of conduction abnormalities such as right or left bundle branch block or complete atrioventricular (AV) block. Here we describe the case of a KSS patient with type I diabetes who experienced syncope in the presence of complete AV block, confirmed by muscular biopsy.
- A 16-year-old boy was first seen in the emergency department with an episode of loss of consciousness. His parents reported that it was the first such episode, no premonitory symptoms had been observed, and there was no notable family history.
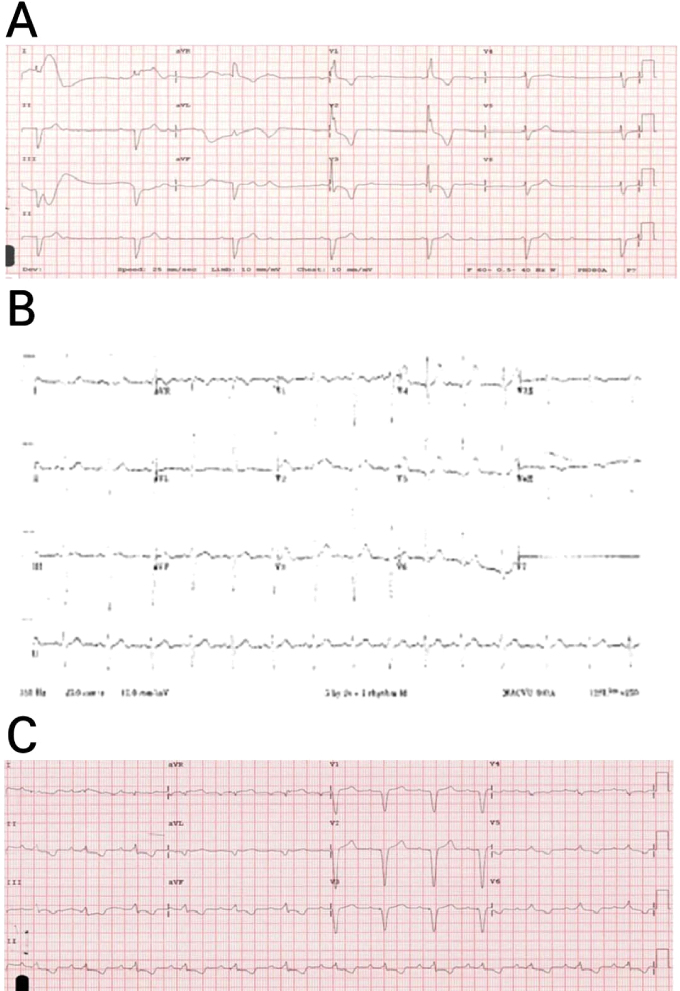
- Physical examination revealed no abnormality and stable vital signs (blood pressure: 110/70 mmHg, respiratory rate: 18 breaths per minute, body temperature: 36.2℃), but the patient's ECG revealed complete AV block with a wide QRS (150 ms), ventricular rhythm was 34 beats per minute, and corrected QT interval was 378 ms (Fig. 1A) Therefore, we performed temporary pacemaker insertion. We observed patients in the intensive care unit (ICU) under continuous ECG monitoring without Holter monitoring.
- The patient had been of short stature since childhood and did not like to exercise because of easy fatigue. At 4 years old, exotropia levator resection and lateral rectus resection were performed to repair what had been considered congenital ptosis. Additionally, median rectus resection was performed when the patient was 10 years old due to subsequent recurrent exotropia. There was no abnormality of the ECG at that time (Fig. 1B). He was diagnosed with type I diabetes and started insulin therapy at 15 years of age. At that time, the HbA1c level was 10.1%, and serum C-peptide levels were 0.221 ng/mg (fasting) and 1.19 ng/mg (postprandial).
- At this time, CBC and ESR were within the normal ranges for the patient's age and sex. Serum lactate (25.2 mg/dl) and myoglobulin levels (150.6 ng/ml) were elevated. Liver function test showed mild elevation, with elevated AST (63 IU/L) and ALT (43 IU/L). Muscle enzymes lactate dehydrogenase (754 IU/L) and creatine phosphokinase (1139 IU/L) were also elevated. Other laboratory findings such as BUN (13.1 mg/dl), creatinine (0.93 mg/dl), Na (141 mEq/L), K (3.4 mEq/L), Ca (8.8 mg/dl), and Mg (2.0 mg/dl) were normal. Thyroid function test was also normal. Left ventricular ejection fraction was 61.1% without regional wall motion abnormality on echocardiography.
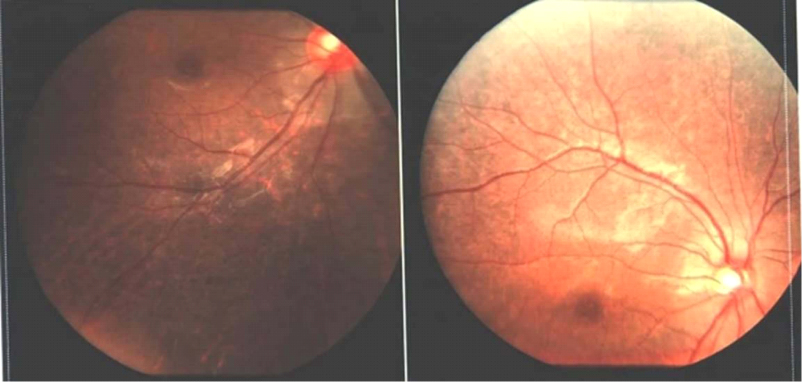
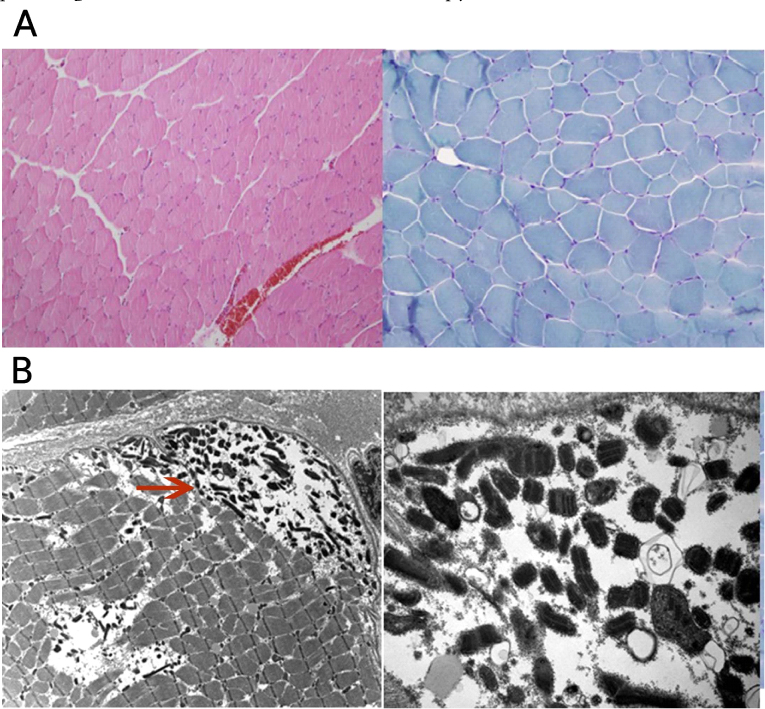
- On ophthalmoscopy to discriminate KSS, the fundus showed atypical retinal pigmentary degeneration (Fig. 2). We impressed mitochondrial myopathy, and biopsy of the right thigh muscle (medial side) was performed. Unexpectedly, on light microscopic examination, modified trichrome stain revealed no diagnostic abnormalities such as ragged red fibers. Other enzyme histochemical and immunohistochemical stains were unremarkable (Fig. 3A), but electron microscopic examination, which is generally considered a more precise examination for mitochondria, revealed muscle cells with subsarcolemmal collections of mitochondria, many of them containing crystalline inclusions, electron microscopically consistent with mitochondrial myopathy (Fig. 3B).
- After 3 days, ECG showed no recovery of normal sinus rhythm and persistent complete AV block, so we inserted a permanent pacemaker (DDDR type) (Fig. 1C). Cardiac MRI performed to exclude structural abnormalities before permanent pacemaker insertion showed normal cardiac chamber size and myocardial wall thickness and no myocardial delayed hyperenhancement, structural abnormality, or myocardial infiltrative disease.
- We finally diagnosed Kearns-Sayre syndrome based on clinical manifestation, laboratory findings, and pathological confirmation.
CASE
- Kearns-Sayre syndrome (KSS) has become recognized as a disease entity comprised of a constellation of features including progressive external ophthalmoplegia, pigmentary retinopathy, cardiac conduction system disorder, and multiple endocrine disorders.3
- Muscle biopsy can confirm the diagnosis based on cytochrome C oxidase-negative ragged red fibers on modified Gomori stain. Electron microscopy reveals subsarcolemmal accumulation of abnormal mitochondria with paracrystalline inclusion bodies, and a more definite diagnosis based on mitochondrial DNA deletions determined by Southern blot or polymerase chain reaction should be sought.6
- Our patient had several characteristic features of KSS, including progressive external ophthalmoplegia, retinal pigmentation, so-called “salt and pepper retinitis”, ptosis, muscle weakness, and mild cognitive disorders as well as type I diabetes (reported to affect 10% of KSS patients.3), metabolic acidosis, and high levels of lactate and creatine kinase. Of these, the cardiac manifestations, which create various degrees of AV block through the His-Purkinje system, are the most important factor for determining the prognosis of the disease.
- In some rare cases, KSS has been diagnosed after death due to cardiac arrest. Most KSS patients have been diagnosed in Europe, the Middle East, and North America.4567 In Korea, one case involving the cardiac conduction system has been reported. That patient had a permanent pacemaker implanted, but the diagnosis was not confirmed by muscle biopsy.8
- Our patient's diagnosis of KSS involving the cardiac conduction system was confirmed by muscle biopsy, which is rarely performed in Korea. In this case, we aimed to prevent sudden cardiac arrest by implanting a pacemaker at an early stage in patients who had specific ECG findings and it is meaningful to make follow up the KSS.
- When we saw the KSS patients, we could detect right or left bundle branch block or complete AV block on ECG, Prophylactic pacemaker therapy is advisable in these patients because of the potential for progression of conduction abnormalities and risk of sudden death.
DISCUSSION
- 1. Duning T, Deppe M, Keller S, Mohammadi S, Schiffbauer H, Marziniak M. Diffusion tensor imaging in a case of Kearns-Sayre syndrome: striking brainstem involvement as a possible cause of oculomotor symptoms. J Neurol Sci 2009;281:110–112.ArticlePubMed
- 2. Chawla S, Coku J, Forbes T, Kannan S. Kearns-Sayre syndrome presenting as complete heart block. Pediatr Cardiol 2008;29:659–662.ArticlePubMed
- 3. Franzese A, Del Giudice E, Santoro L, De Filippo G, Argenziano A. Diabetes mellitus in Kearns-Sayre syndrome: a case with a 10-year follow-up. Diabetes Res Clin Pract 1995;30:233–235.ArticlePubMed
- 4. Riera AR, Kaiser E, Levine P, Schapachinik E, Dubner S, Ferreira C, et al. Kearns-Sayre syndrome: electro-vectorcardiographic evolution for left septal fascicular block of the his bundle. J Electrocardiol 2008;41:675–678.ArticlePubMed
- 5. Yorifuji S, Ogasahara S, Takahashi M, Tarui S. Decreased activities in mitochondrial inner membrane electron transport system in muscle from patients with Kearns-Sayre syndrome. J Neurol Sci 1985;71:65–75.ArticlePubMed
- 6. Tranchant C, Mousson B, Mohr M, Dumoulin R, Welsch M, Weess C, et al. Cardiac transplantation in an incomplete Kearns-Sayre syndrome with mitochondrial DNA deletion. Neuromuscul Disord 1993;3:561–566.ArticlePubMed
- 7. Puri A, Pradhan A, Chaudhary G, Singh V, Sethi R, Narain VS. Symptomatic complete heart block leading to a diagnosis of Kearns-Sayre syndrome. Indian heart J 2012;64:515–517.ArticlePubMedPMC
- 8. Park IH, Lim JK, Moon JG, Joung BY, Lee MH, Kim SS. A Case of Kearns Sayre syndrome complicated with complete AV block. Korean J Med 2006;70:564–568.
References
Fig. 1
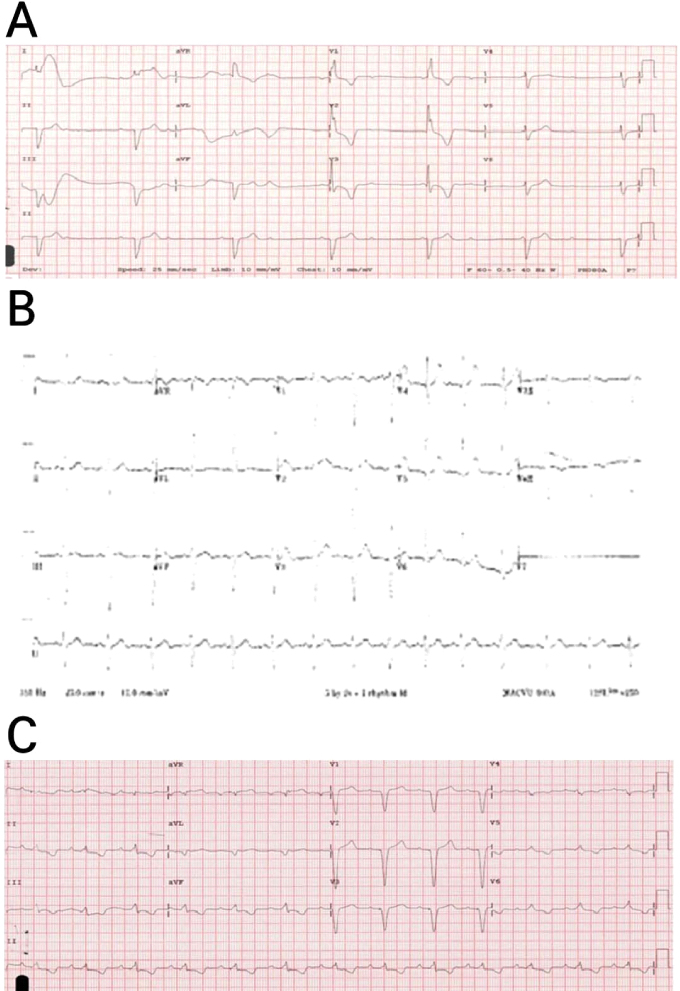
ECG revealed complete atrioventricular block with a wide QRS (150 ms) and ventricular rhythm of 34 beats per minute (bpm) (A), normal finding at 9 years old (B), and pacemaker rhythm(DDDR type). (C).
Fig. 2
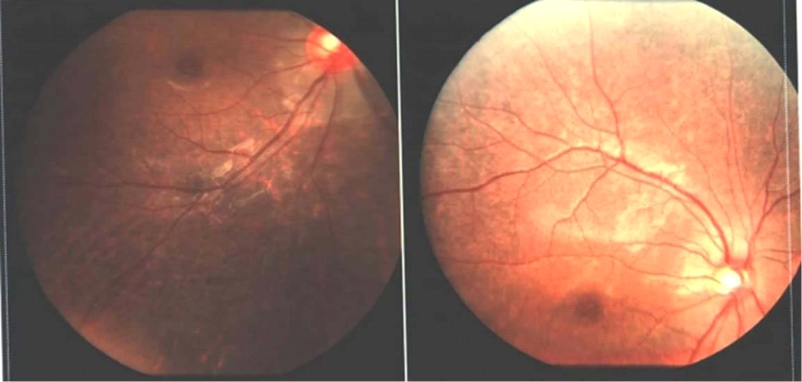
Ophthalmoscopy of the fundus showed atypical retinal pigmentary degeneration (salt and pepper retinitis) (red arrow).
Fig. 3
Modified trichrome stain revealed no diagnostic abnormalities such as ragged red fibers, similar to other enzyme histochemical and immunohistochemical stains (A, LM finding), but showed muscle cells with subsarcolemmal collection of mitochondria, many of them containing crystalline inclusions (red arrow), electron microscopically consistent with mitochondrial myopathy (B, EM finding).
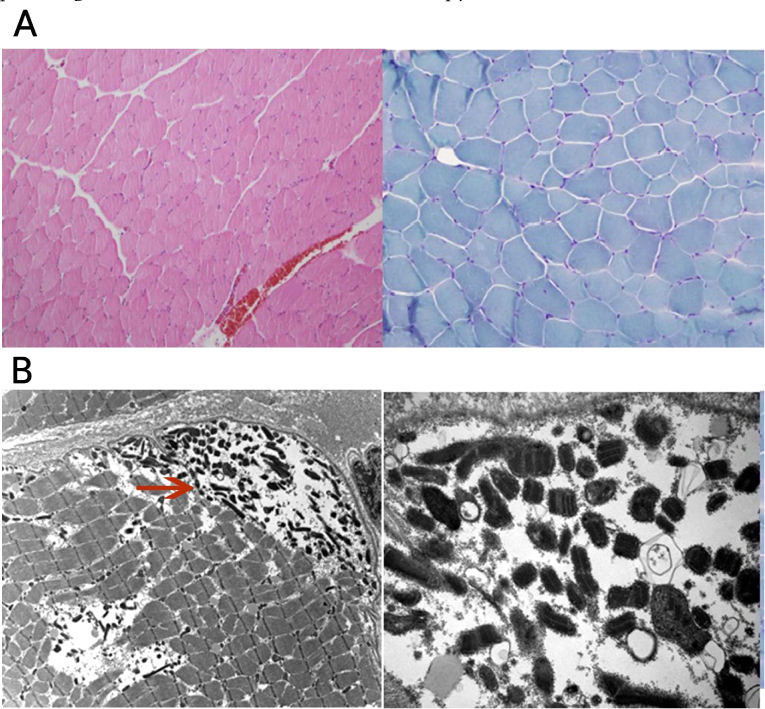
Light and electron microscopic examination of the right thigh muscle
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite