 KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 35(1); 2020 > Article
-
Original Articles
Expressions of miRNAs in Papillary Thyroid Carcinoma and Their Associations with the BRAFV600E Mutation and Clinicopathological Features - Song I Yang, Young Sik Choi
-
Kosin Medical Journal 2020;35(1):1-14.
DOI: https://doi.org/10.7180/kmj.2020.35.1.1
Published online: June 30, 2020
1Department of Surgery, College of Medicine, Kosin University, Busan, Korea
2Department of Internal Medicine, College of Medicine, Kosin University, Busan, Korea
- Corresponding Author: Song I Yang, Department of Surgery, College of Medicine, Kosin University, 262, Gamcheon-ro, seo-gu, Busan 49267, Korea, Tel: +82-51-990-6721, Fax: +82-246-6093, E-mail: tonybin@daum.net
Copyright © 2020 by Korean Association of Medical Journal Editors
Articles published in Kosin Medical Journal are open-access, distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,003 Views
- 16 Download
- 1 Crossref
Abstract
-
Objectives
- The microRNAs (miRNAs) are known to be commonly expressed in papillary thyroid carcinoma. The BRAFV600E mutation is the most common genetic mutation in thyroid cancer. The main aim of this study was to determine the possible association between expression of the three miRNAs and that of BRAFV600E mutation and the clinicopathological features in papillary thyroid carcinoma.
-
Methods
- This study was conducted on 51 paraffin-embedded tissues (42 thyroid cancer, 9 benign tumor) obtained from patients undergoing thyroidectomy at the Endocrine Center of OOO University Hospital.
-
Results
- miRNAs expression was significantly high in patients with cervical lymph node metastasis and advanced TNM stage. In addition, miR-146b expression levels were significantly higher in papillary thyroid carcinoma patients with BRAFV600E mutation. The relative quantification (2-ΔΔCt) of miR-146b was also high among the miRNAs. Individually, the AUCs for miRNA-146b was 0.923 (cutoff value −1.97, sensitivity 88.9%, specificity 85.7%).
-
Conclusions
- Especially, expression of miR-146b increased higher in PTC patients with BRAFV600E mutation. These findings showed a role of miR-146b as potential biomarkers in differentiating PTC from benign tumor and as a prognostic indicator of PTCs. Further investigation will need for the roles of miRNAs in the pathogenesis of papillary thyroid carcinomas.
- Subjects
- This study was conducted on portions of paraffin-embedded tissues obtained from patients who had undergone thyroidectomy at the Endocrine Center of the Kosin University Gospel Hospital. Tissues were obtained from a total of 51 cases; among these, 42 cases involved thyroid cancer and 9 cases involved benign tumor. The mean age of the patients was 47.1 ± 11.2 years (range 28 – 75 years), and the male to female ratio was 1:4.3. This study was approved by the Institutional Review Board of Kosin University Gospel Hospital.
- Methods
- The American Joint Committee on Cancer Staging System for differentiated cancers published in 201619 was used to classify patients who were 55 years or younger and had TMN stage 1 or were older than 55 years and had TMN stage 1 or 2 into the low-risk group. The remaining patients were classified into the high-risk group.
- This study has been approved by the Institutional Review Board of the Kosin University Gospel Hospital (approval no. 2014-10-140).
- Genomic DNA was extracted using the QIAamp DNA FFPE Tissue kit (Qiagen, Hilden, Germany), from paraffin-embedded tumor tissues that were cut to a thickness of 10 μm and were obtained from patients subjected to thyroidectomy.
- The DNA was amplified by adding 50 ng of DNA to a mixture containing 10 μL 2X concentrated HotStarTaq Master Mix (Qiagen), 3 mM MgCl2, 0.3 μM primer pairs, and 400 μM deoxynucleotide triphosphate. The amplification of BRAF exon 15 was performed using the forward and reverse Exon 15 primers: forward, 5′-atgcttgctctgataggaaaatga-3′; reverse, 5′-agcagcatctcagggcca-3′. The PCR reaction conditions were set as follows: 35 repeats of 30 s at 94°C, 30 s at 58°C, and 45 s at 72°C, and a final extension for 10 min at 72°C.
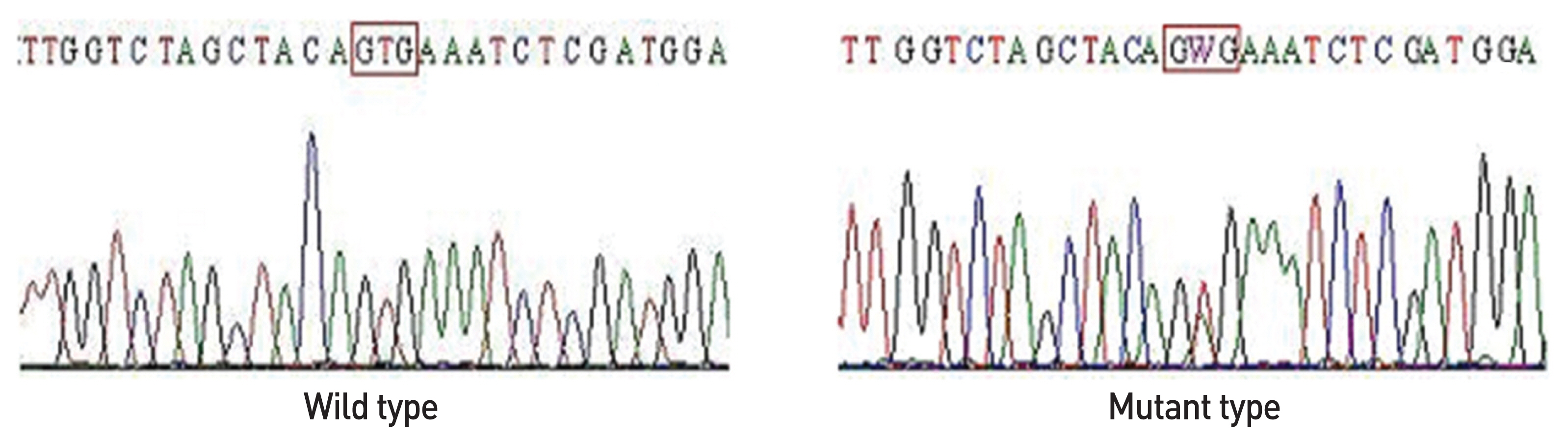
- DNA was purified from a slice of the 2% agarogel (used for electrophoresis) using the QIAgen gel extraction kit (Qiagen). The purified product was amplified using fluorescence-activated ddNTP (BigDye3.1; Applied Biosystems, Foster City, CA, USA); subsequently, ethanol was used for purification. The purified product was dissolved in 10μL HiDi-Formamide, and the solution analyzed using an ABI PRISM 3100 automated capillary DNA sequencer (Applied Biosystems) (Fig. 1).
- Total RNA was separated from the paraffin-embedded tissues; the paraffin tissue was placed in an RNase-free tube to which 300 μL melting buffer was added. This was centrifuged and incubated at 72°C for 10 min. Subsequently, 20 μL of proteinase K solution was added to this solution. The extract was mixed with 400 μL of binding buffer and 800 μL of 100% ethanol at 60°C. Following this, a cartridge was placed within the collection tube in order to transfer 700 μL of the extract containing the binding buffer and ethanol; this was then centrifuged twice. Five hundred microliters of the wash buffer and 100% ethanol were added to the cartridge and centrifuged; this process was performed in triplicate, and the final solution discarded. RNAse-free DW (50 μL) at 65°C was added to the cartridge; the tube was incubated for 1 min, and subsequently centrifuged. The total RNA remaining in the tube following the removal of the cartridge was used in further experiments.
- The miR-221, miR-222, and miR-146b microRNA expression was measured using the Taq-Man miRNA assay. Two microliters of the synthesized cDNA was subjected to quantitative real time PCR, using the ABI PRISM 7000 sequence detection system (Applied Biosystems). The cDNA was mixed with a 20 μL solution containing 10 μL TaqMan 2X universal PCR master mix (Applied Biosystems), 1 μL of the primer and probe mix (20X), and 7 μL RNase free water. As a double analysis, the level of miRNA expression was measured. U6 small RNA (RNU6B) was quantified as the standardized control group for the target miRNA. The same sample was used to perform quantitative real time PCR three times, in order to obtain the mean value for quantifying the level of expression. The threshold cycle value (Ct value) of each PCR reaction, generated using the RNU6B expression as a reference, was standardized. The standardized values were converted to relative values. The relative quantity of miRNA for each sample was calculated as ΔCt, which was the value obtained by subtracting the Ct value of RNU6B (used as the endogenous control) from the Ct value of the sample. The relative quantification of gene expression between the malignant and benign tumors was calculated via the 2−ΔΔCt method (Applied Biosystems user bulletin no. 2 (P/N 4303859)), using the ΔΔCt value (difference between the ΔCt value exhibited by papillary thyroid carcinoma patients and the ΔCt value of benign nodes).
- Statistical analysis
- The clinicopathological features of the subjects were demonstrated using the independent t-test and chi-square test. The changes in miRNA expression were displayed as mean ± standard deviation (SD). The differences in miRNA expression between benign and malignant nodes were compared by independent t-test, and the differences between the expression of various miRNAs were analyzed by one-way analysis of variance (ANOVA); a post-hoc test was performed using the Scheffe’s method. A ROC (receiver operating characteristic) curve analysis was performed in order to assess the possibility of using miR-221, miR-222, and miR-146b as diagnostic biomarkers for papillary carcinoma. The SPSS (version 18.0; IBM, Armonk, NY, USA) software was used for statistical analysis, and the significance level was set to P < 0.05.
METRIALS AND METHODS
1) Classification of risk groups
2) BRAFV600E mutation analysis
(1) DNA extraction
(2) Amplification
(3) Direct sequencing
3) Expression of miRNA-146 b, miRNA-221, and miRNA-222
(1) RNA extraction
(2) Quantitative real time polymer chain reaction (qRT-PCR)
- Clinicopathological features of papillary carcinoma
- The mean tumor size observed in the 42 papillary carcinoma test subjects was 15.2 ± 9.9 mm; 23 of these cases (54.7%) tested positive for the BRAFV600E mutation. We also observed 22 cases (52.4%) of extrathyroidal extension, 22 cases (52.4%) of lymph node metastasis, 27 cases (64.3%) of low-risk TMN staging group, and 15 cases (35.7%) of high-risk TMN staging group (Table 1).
- Association between miR-221, miR-222, and miR-146b expression and the clinicopathological features of papillary thyroid carcinomas
- miR-221 expression was high in the lymph node metastasis (P = 0.00) high-risk TMN staging group (P = 0.00); in addition, miRNA-222 and miRNA-146b expression was significantly high in cases displaying a tumor size ≥ 1 cm (P = 0.02), extrathyroidal extension (P = 0.00), lymph node metastasis (P = 0.01), and the high-risk TMN staging group (P = 0.00). In particular, miRNA-146b expression was significantly elevated in the group expressing the BRAFV600E mutation, compared to the group without the mutation (P = 0.02) (Table 2).
- Comparing the miR-221, miR-222, and miR-146b expression in benign and malignant tumors
- The mean ΔCt values of miR-221, miR-222, and miR-146b in benign tumor cases were −0.11 ± 1.65, −1.65 ± 1.31, and −0.09 ± 1.61, respectively; on the other hand, the mean ΔCt values of miR-221, miR-222, and miR-146b observed in papillary carcinoma cases were −1.75 ± 1.62, −4.17 ± 1.53, and −3.71 ± 1.98, respectively. The ΔCt values for all 3 miRNA were significantly elevated in papillary carcinoma cases, compared to the benign tumor cases (P = 0.00) (Fig. 2).
- In terms of the differences in expression between the different types of miRNA, miR-222 and miR-146b showed a significantly elevated expression compared to miR-221 (P = 0.00); however, no significant differences were observed between miR-222 and miR-146b (Fig. 2).
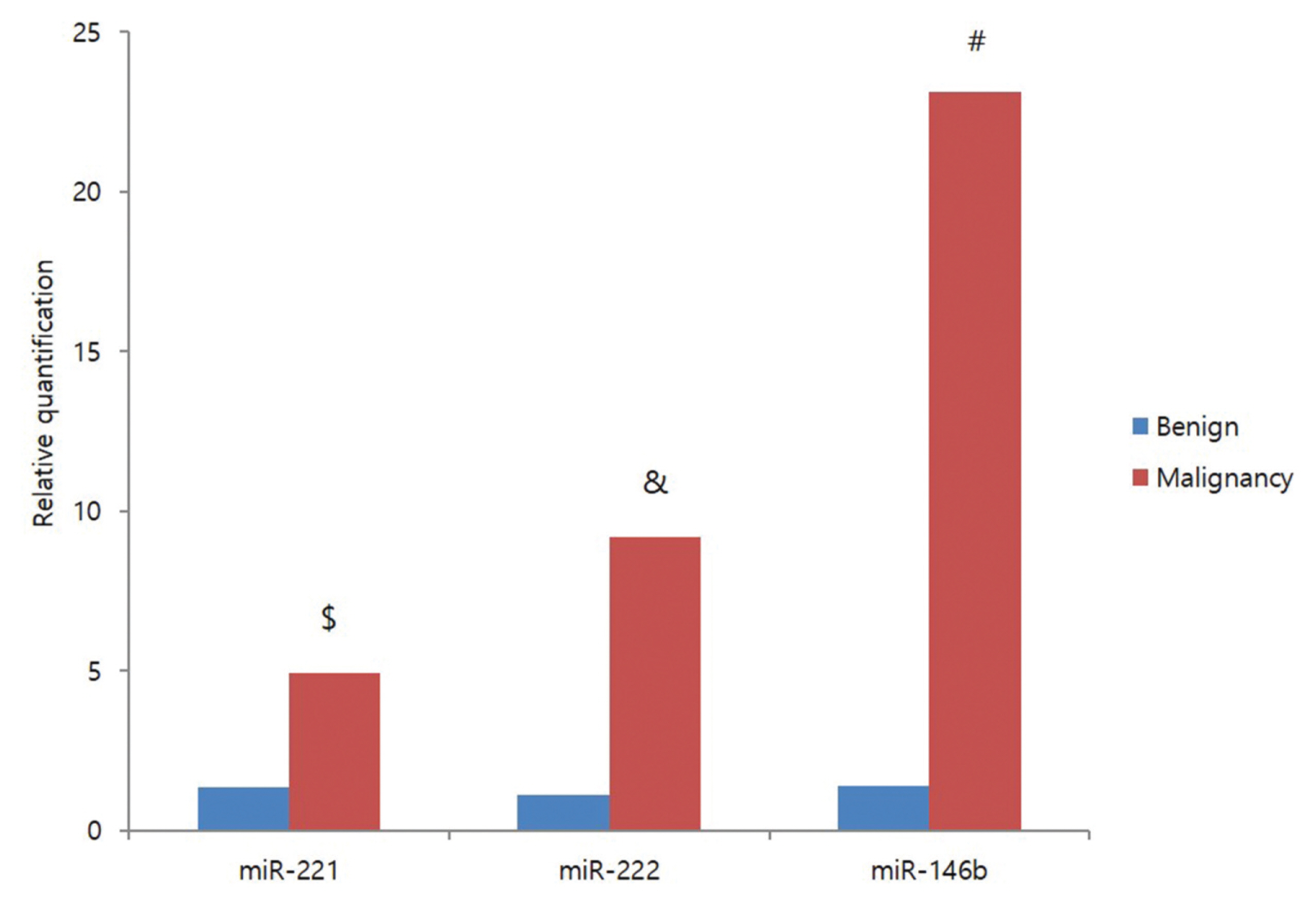
- The relative quantification (2−ΔΔCt) revealed that genetic (microRNA) expression was significantly higher in malignant tumors than in benign tumors (P = 0.00). The 2−ΔΔCt values for miR-221, miR-222, and miR-146b expression in papillary carcinoma were 4.91 ± 8.31, 9.18 ± 20.14, and 23.13 ± 28.59, respectively; this indicated that the 2−ΔΔCt value of miR-146b was significantly higher than that of miR-221 or miR-222 (P = 0.00). However, no significant differences were observed between miR-221 and miR-222 (Fig. 3).
- ROC curve analysis of miR-221, miR-222, and miR-146b expression in benign tumor and papillary carcinoma
- The diagnostic value of miR-221, miR-222, and miR-146b for papillary thyroid carcinoma was assessed by performing an ROC curve analysis. miR-221 showed an area under the curve (AUC) of 0.762 (95% CI; 0.591 – 0.932), a cutoff value of −0.93, and a sensitivity and specificity of 77.8% and 69.0%, respectively. miR-222 showed an AUC of 0.903 (95% CI; 0.803–1), cutoff value of −3.03, and sensitivity and specificity of 88.9% and 81.0%, respectively. miR-146b showed an AUC of 0.923 (95% CI; 0.849–0.998), a cutoff value, sensitivity, and specificity of −1.97, 88.9%, and 85.7%, respectively (Fig. 4).
RESULTS
- In this study investigating the miRNAs miR-221, miR-222, and miR-146b, and BRAFV600E mutation (whose expression is commonly enhanced in papillary thyroid carcinoma), there was a significant increase in all miRNA in papillary carcinoma, compared to the benign tumor. The study conducted by Sun et al.20, which investigated miR-221, miR-222, miR-146b, miR-181, and miR-21, reported a significant increase in the miR-221 and miR-222 expression in the lymph node metastasis and high-risk TMN staging group. Chou et al.17 demonstrated that, although the expression of the miRNAs miR-221, miR-222, and miR-146b were elevated in the high-risk TMN staging group, no differences were seen between the patients with or without lymph node metastasis. In this study, all three miRNAs, miR-221, miR-222, and miR-146b, showed high levels of expression in the lymph node metastasis and high-risk TMN staging group; miR-222 and miR-146b expression was significantly increased in the extrathyroidal extension, with a tumor size ≥ 1 cm. This demonstrated the association of miRNA expression with the clinicopathological features of tumors. With the increase in prevalence of ultrasound testing, a greater number of cases of thyroidal nodules are being discovered; fine needle aspiration cytology is used in the diagnosis of these thyroidal nodules. However, shortcomings such as insufficient specimens, unconfirmed diagnosis, and/or false negative results have led to the demand for a new diagnostic method.21 Gene detection technology has advanced significantly over the past 10 years. This has allowed for the analysis of tumorigenesis and progression of papillary thyroid carcinoma at a molecular biology level, as well as the development of biomarkers for diagnosis and prediction papillary thyroid carcinoma prognosis. Among the currently available genetic technologies, specific miRNAs (and their expression) can be applied as potential molecular biology biomarkers for papillary thyroid carcinoma. Sun et al.22, who used 5 miRNA (miR-221, miR-222, miR-146b, miR-181, and miR-21) expressed in thyroid tumors, reported that miRNA-146b had the highest diagnostic value, with sensitivity, specificity, and AUC of 90.4%, 88.9%, and 0.952, respectively. This demonstrated its potential use as a potential biomarker in order to discriminate between benign and malignant tumors. Our study also showed miRNA-146b to have the highest diagnostic value with 88.9% sensitivity, 85.7% specificity, and an AUC of 0.923. Moreover, the relative quantification (2−ΔΔCt) of genetic expression between benign and malignant tumors revealed that miR-146b expression was higher than that of miR-221 or miR-222; in addition, the positive results for the BRAFV600E mutation were also related to miR-146b. Chou et al.18, based on the results of a multivariate logistic regression analysis, reported that in addition to being an indicator of cervical lymph node metastasis and the stage of tumor, miR-146b expression was an independent risk factor indicating the poor prognosis of papillary carcinoma. Furthermore, higher miR-146b expression levels were associated with a notably lower overall survival rate, compared to cases with lower levels of expression; the hazard ratio was also 3.92 times higher.
- The target genes regulated by miR-146b, and the molecular mechanism by which miR-146b influences the aggressiveness of tumor cells in papillary carcinoma are not well known. However, Geraldo et al.22 reported that miR-146b induced the expression of SMAD4 in order to regulate the signal pathway of transforming growth factor (TGF)-β in thyroid tumorigenesis; additionally, they stated that the over-expression of miR-146b in PCCL3 cells triggered cell proliferation even in the absence of thyroid stimulating hormone (TSH). In addition to papillary thyroid carcinoma, miR-146b is expressed in other solid tumors. The expression of the BRCA1 gene in a breast cancer cell line was down-regulated by miR-146b, resulting in increased cell proliferation. 23 miR-146b is also associated with poor prognosis in oral squamous cell carcinoma.24
- The BRAFV600E mutation is capable of propagating tumorigenesis in the thyroid of transgenic mice25; this mutation was responsible for the increase in the invasion of thyroid cells in a study using a thyroid cell line.26 Temporary injection of small interfering RNA (siRNA) into a papillary carcinoma cell line with the BRAF mutation (to suppress BRAF) led to the suppression of cell growth and proliferation.27 Although very few studies have been conducted on the BRAF mutation and miRNA expression in papillary thyroid carcinoma, the results of these were shown to be contradictory. Chou et al.17 reported that the BRAFV600E mutation resulted in over-expression of miR-146b; Yip et al.28 also stated that papillary thyroid carcinoma displaying the BRAFV600E mutation led to the over-expression of miR-146b, which was in turn associated with aggressive behavior. Our study also observed the over-expression of miR-146b in the group displaying the BRAFV600E mutation. On the other hand, Sheu et al.29 stated that the BRAFV600E mutation and expression of the miRNA set (miR-221, miR-222, miR-146b, miR-181, and miR-21) were unrelated to each other. In cases with the BRAFV600E mutation, a study conducted by Sun et al.20 revealed significantly high expression of miR-221, miR-222, miR-146b, and miR-181, while another study by Huang et al.30 revealed high expression of miR-21 and miR-203; however, these were attributed to the differences in specimens and examination methods.
- In conclusion, miR-221, miR-222, and miR-146b showed high levels of expression in the lymph node metastasis and high-risk TMN staging group in our study; therefore, miRNA expression was associated with the clinicopathological features of this tumor. In addition, miR-146b showed the highest sensitivity and specificity among the three miRNAs. Moreover, miR-146b expression was demonstrated to be significantly increased in the presence of the BRAFV600E mutation; therefore, miR-146b was believed to be a potential biomarker for the diagnosis of papillary carcinoma. Based on this study, the mutual association between the BRAFV600E mutation and miRNA must be studied further, in order to determine the causes and progression of papillary carcinoma.
- This study was conducted to examine the probable association between expression of miR-221, miR-222, and miR-146b and that of the BRAFV600E mutation and the clinicopathological features in papillary thyroid carcinoma. miR-221, miR-222, and miR-146b expression was high in the lymph node metastasis and high-risk TMN staging group, which indicated the association of miRNA expression with the clinicopathological features. All miRNAs showed significantly elevated expression in papillary carcinoma compared to benign tumor, with miR-221 showing the lowest level of expression among the miRNAs. miR-146b exhibited the highest sensitivity (88.9%), specificity (85.7%), and AUC (0.923), and was believed to show the most diagnostic value as a potential biomarker for differentiating between benign and malignant tumors. Moreover, miR-146b expression was significantly elevated in the presence of the BRAFV600E mutation. This study indicated the potential of miR-146b to be used as a biomarker for diagnosis of papillary carcinoma (in the future).
DISCUSSION


| Clinicopathologic features (n = 42) | miR-221 | miR-222 | miR-146b | |||
|---|---|---|---|---|---|---|
|
|
||||||
| −ΔCTa | P-value | −ΔCT | P-value | −ΔCT | P-value | |
| Age | ||||||
| < 55 years (n = 18) | 1.36 | 0.18 | 3.78 | 0.16 | 3.59 | 0.73 |
| ≥ 55 years (n = 24) | 2.04 | 4.45 | 3.79 | |||
| Gender | ||||||
| Male (n = 8) | 2.31 | 0.28 | 4.62 | 0.36 | 4.83 | 0.06 |
| Female (n = 34) | 1.61 | 4.06 | 3.44 | |||
| Tumor size | ||||||
| ≤ 10 mm (n = 15) | 7.61 | 0.02 | 3.21 | 0.02 | 2.17 | 0.00 |
| > 10 mm (n = 27) | 2.29 | 4.69 | 4.56 | |||
| Capsular invasion | ||||||
| No (n = 20) | 7.52 | 0.00 | 3.34 | 0.00 | 2.62 | 0.00 |
| Yes (n = 22) | 2.65 | 4.92 | 4.69 | |||
| Multifocality | ||||||
| Single (n = 24) | 1.08 | 0.00 | 3.78 | 0.05 | 3.37 | 0.19 |
| Multiple (n = 18) | 2.94 | 4.68 | 4.14 | |||
| BRAFV600E mutation | ||||||
| Negative (n = 19) | 1.56 | 0.49 | 3.98 | 0.47 | 2.94 | 0.02 |
| Positive (n = 23) | 1.90 | 4.32 | 4.34 | |||
| Nodal metastasis | ||||||
| Negative (n = 20) | 1.04 | 0.00 | 3.56 | 0.01 | 2.65 | 0.00 |
| Positive (n = 22) | 2.38 | 4.69 | 4.66 | |||
| Tumor stagingb | ||||||
| Low risk (n = 27) | 1.08 | 0.00 | 1.09 | 0.00 | 3.06 | 0.00 |
| High risk (n = 15) | 2.94 | 2.94 | 4.86 | |||
All data have been presented as mean values.
a −ΔCT = (CtmiRNA − CtU6).
b The low-risk group was defined as comprising patients who were younger than 55 years and had stage I PTC and those aged 55 years or greater with stage I or II PTC, according to the AJCC. The remaining patients were included in the high-risk group.
miRNA, micro RNA; Ct, threshold cycle.
- 1. Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA 2006;295:2164–7.ArticlePubMed
- 2. Ruegemer JJ, Hay ID, Bergstralh EJ, Ryan JJ, Offord KP, Gorman CA. Distant metastases in differentiated thyroid carcinoma: a multivariate analysis of prognostic variables. J Clin Endocrinol Metab 1988;67:501–8.ArticlePubMed
- 3. Xing M, Westra WH, Tufano RP, Cohen Y, Rosenbaum E, Rhoden KJ, et al. BRAF mutation predicts a poorer clinical prognosis for papillary thyroid carcinoma. J Clin Endocrinol Metab 2005;90:6373–9.PubMed
- 4. Kebebew E, Weng J, Bauer J, Ranvier G, Clark OH, Duh QY, et al. The prevalence and prognostic value of BRAF mutation in thyroid cancer. Ann Surg 2007;246:466–70.ArticlePubMedPMC
- 5. Kim SW, Lee JI, Kim JW, Ki CS, Oh YL, Choi YL, et al. BRAFV600E mutation analysis in fine-needle aspiration cytology specimens for evaluation of thyroid nodule: a large series in a BRAFV600E-prevalent population. J Clin Endocrinol Metab 2010;95:3693–700.ArticlePubMed
- 6. Xing M. BRAF mutation in papillary thyroid cancer: pathogenic role, molecular bases, and clinical implications. Endocr Rev 2007;28:742–62.ArticlePubMed
- 7. Namba H, Nakashima M, Hayashi T, Hayashida N, Maeda S, Rogounovitch TI, et al. Clinical implication of hot spot BRAF mutation, V599E, in papillary thyroid cancers. J Clin Endocrinol Metab 2003;88:4393–7.ArticlePubMed
- 8. Ito Y, Yoshida H, Maruo R, Morita S, Takano T, Hirokawa M, et al. BRAF mutation in papillary thyroid carcinoma in a Japanese population: its lack of correlation with high-risk clinicopathological features and disease-free survival of patients. Endocr J 2009;56:89–97.ArticlePubMed
- 9. Zeng Y. Principles of micro-RNA production and maturation. Oncogene 2006;25:6156–62.ArticlePubMed
- 10. Hammond SM, Boettcher S, Caudy AA, Kobayashi R, Hannon GJ. Argonaute2, a link between genetic and biochemical analyses of RNAi. Science 2001;293:1146–50.ArticlePubMed
- 11. Esquela-Kerscher A, Slack FJ. Oncomirs-microRNAs with a role in cancer. Nat Rev Cancer 2006;6:259–69.ArticlePubMedPDF
- 12. Dalmay T, Edwards DR. MicroRNAs and the hallmarks of cancer. Oncogene 2006;25:6170–5.ArticlePubMed
- 13. Chen YT, Kitabayashi N, Zhou XK, Fahey TJ 3rd, Scognamiglio T. MicroRNA analysis as a potential diagnostic tool for papillary thyroid carcinoma. Mod Pathol 2008;21:1139–46.ArticlePubMed
- 14. He H, Jazdzewski K, Li W, Liyanarachchi S, Nagy R, Volinia S, et al. The role of microRNA genes in papillary thyroid carcinoma. Proc Natl Acad Sci U S A 2005;102:19075–80.ArticlePubMedPMC
- 15. Nikiforova MN, Tseng GC, Steward D, Diorio D, Nikiforov YE. MicroRNA expression profiling of thyroid tumors: biological significance and diagnostic utility. J Clin Endocrinol Metab 2008;93:1600–8.ArticlePubMedPMC
- 16. Cahill S, Smyth P, Denning K, Flavin R, Li J, Potratz A, et al. Effect of BRAFV600E mutation on transcription and post-transcriptional regulation in a papillary thyroid carcinoma model. Mol Cancer 2007;6:21–30.ArticlePubMedPMCPDF
- 17. Chou CK, Chen RF, Chou FF, Chang HW, Chen YJ, Lee YF, et al. miR-146b is highly expressed in adult papillary thyroid carcinomas with high risk features including extrathyroidal invasion and the BRAFV600E mutation. Thyroid 2010;20:489–94.ArticlePubMed
- 18. Chou CK, Yang KD, Chou FF, Huang CC, Lan YW, Lee YF, et al. Prognostic implications of miR-146b expression and its functional role in papillary thyroid carcinoma. J Clin Endocrinol Metab 2013;98:196–205.Article
- 19. Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK, et al. AJCC Cancer Staging Manual. 8th ed. New York (NY): Springer; 2016.
- 20. Sun Y, Yu S, Liu Y, Wang F, Liu Y, Xiao H. Expression of miRNAs in Papillary Thyroid Carcinomas Is Associated with BRAF Mutation and Clinicopathological Features in Chinese Patients. Int J Endocrinol 2013;128:735.ArticlePDF
- 21. Nga ME, Kumarasinghe MP, Tie B, Sterrett GF, Wood B, Walsh J, et al. Experience with standardized thyroid fine needle aspiration reporting categories: follow-up data from 529 cases with ‘indeterminate’ or ‘atypical’ reports. Cancer Cytopathol 2010;118:423–33.PubMed
- 22. Geraldo MV, Yamashita AS, Kimura ET. MicroRNA miR-146b-5p regulates signal transduction of TGF-β by repressing SMAD4 in thyroid cancer. Oncogene 2012;31:1910–22.ArticlePubMed
- 23. Garcia AI, Buisson M, Bertrand P, Rimokh R, Rouleau E, Lopez BS, et al. Down-regulation of BRCA1 expression by miR-146a and miR-146b-5p in triple negative sporadic breast cancers. EMBO Mol Med 2011;3:279–90.ArticlePubMedPMC
- 24. Scapoli L, Palmieri A, Lo Muzio L, Pezzetti F, Rubini C, Girardi A, et al. microRNA expression profiling of oral carcinoma identifies new markers of tumor progression. Int J Immunopathol Pharmacol 2010;23:1229–34.ArticlePubMed
- 25. Knauf JA, Ma X, Smith EP, Zhang L, Mitsutake N, Liao XH, et al. Targeted expression of BRAFV600E in thyroid cells of transgenic mice results in papillary thyroid cancers that undergo dedifferentiation. Cancer Res 2005;65:4238–45.ArticlePubMed
- 26. Melillo RM, Castellone MD, Guarino V, De Falco V, Cirafici AM, Salvatore G, et al. The RET/PTC-RAS-BRAF linear signaling cascade mediates the motile and mitogenic phenotype of thyroid cancer cells. J Clin Invest 2005;115:1068–81.ArticlePubMedPMC
- 27. Salvatore G, DeFalco V, Salerno P, Nappi TC, Pepe S, Troncone G, et al. BRAF is a therapeutic target in aggressive thyroid carcinoma. Clin Cancer Res 2006;12:1623–9.ArticlePubMed
- 28. Yip L, Kelly L, Shuai Y, Armstrong MJ, Nikiforov YE, Carty SE, et al. MicroRNA Signature Distinguishes the Degree of Aggressiveness of Papillary Thyroid Carcinoma. Ann Surg Oncol 2011;18:2035–41.ArticlePubMedPMC
- 29. Sheu SY, Grabellus F, Schwertheim S, Handke S, Worm K, Schmid KW. Lack of correlation between BRAF V600E mutational status and the expression profile of a distinct set of miRNAs in papillary thyroid carcinoma. Horm Metab Res 2009;41:482–7.ArticlePubMed
- 30. Huang Y, Liao D, Pan L, Ye R, Li X, Wang S, et al. Expressions of miRNAs in papillary thyroid carcinoma and their associations with the BRAFV600E mutation. Eur J Endocrinol 2013;15 168:675–81.ArticlePubMed
References
Figure & Data
References
Citations
- Cyto-Histological Profile of MicroRNAs as Diagnostic Biomarkers in Differentiated Thyroid Carcinomas
Maria de Lurdes Matos, Mafalda Pinto, Marta Alves, Sule Canberk, Ana Gonçalves, Maria João Bugalho, Ana Luísa Papoila, Paula Soares
Genes.2024; 15(3): 389. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite



