 KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 32(2); 2017 > Article
-
Review Article
The early diagnosis and treatments in multiple sclerosis - So Young Huh
-
Kosin Medical Journal 2017;32(2):151-163.
DOI: https://doi.org/10.7180/kmj.2017.32.2.151
Published online: January 19, 2017
Department of Neurology, College of Medicine, Kosin University, Busan, Korea
- Corresponding Author: So Young Huh, Department of Neurology, College of Medicine, Kosin University, 262, Gamcheon-ro, Seo-gu, Busan 49267, Korea Tel: +82-51-990-6461 Fax: +82-51-990-3077 E-mail: caccu@naver.com
• Received: April 6, 2017 • Accepted: April 19, 2017
Copyright © 2017 Kosin University School of Medicine Proceedings
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 765 Views
- 4 Download
Abstract
- Multiple sclerosis (MS) is a chronic inflammatory demyelinating disorder of the central nervous system that leads to neurological disability. The diagnosis of MS relies on the MRI criteria, which can demonstrate dissemination in space and time. Exclusion of other demyelinating mimics is essential because there are no specific biomarker for MS and MRI criteria are still have imperfect. There is incremental improvements in MS treatment option that have contributed to the delay of disease progression. The early initiation of DMT may ameliorate the neurological disability. In this review, we discusses the new diagnostic MS criteria and summarize the evidences supporting the early treatment in the course of MS.
Fig. 1.Example of lesion for multiple sclerosis MRI Criteria of dissemination in space (A) periventricular lesions; (B) juxtacortical lesions; (C) infratentorial lesions; (D) spinal cord lesion; (E) optic nerve lesion. Gadolinium-enhancing lesion in T1 gadolinium weighted image; (F) are visible in the patient with MS.
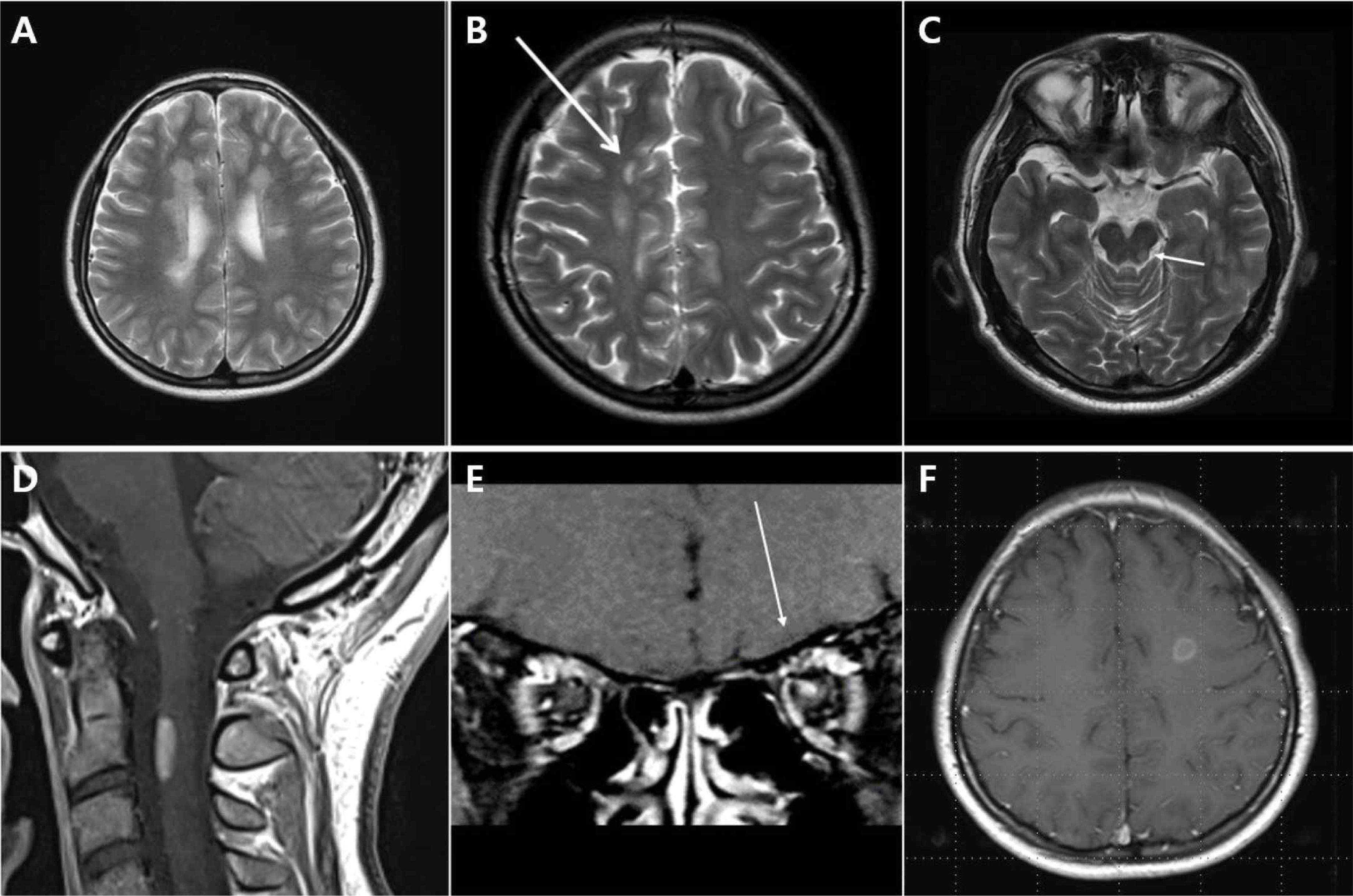
Table 1.CIS clinical features and likelihood of signaling an MS diagnosis4
Table 2.2010 McDonald criteria and 2016 MAGNIMS Diagnosis criteria8
Table 3.Clinical and MRI major red flags suggestive of alternative diagnosis to multiple sclerosis4
- 1.Compston A, Coles A. Multiple sclerosis. Lancet 2008;372:1502–17.ArticlePubMed
- 2.Miller DH, Chard DT, Ciccarelli O. Clinically isolated syndromes. Lancet Neurol 2012;11:157–69.ArticlePubMed
- 3.Miller D, Barkhof F, Montalban X, Thompson A, Filippi M. Clinically isolated syndromes suggestive of multiple sclerosis, part I: natural history, pathogenesis, diagnosis, and prognosis. Lancet Neurol 2005;4:281–8.ArticlePubMed
- 4.Miller DH, Weinshenker BG, Filippi M, Banwell BL, Cohen JA, Freedman MS, et al. Differential diagnosis of suspected multiple sclerosis: a consensus approach. Mult Scler 2008;14:1157–74.ArticlePubMedPMC
- 5.McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann Neurol 2001;50:121–7.ArticlePubMed
- 6.Polman CH, Reingold SC, Edan G, Filippi M, Hartung HP, Kappos L, et al. Diagnostic criteria for multiple sclerosis: 2005 revisions to the “McDonald Criteria”. Ann Neurol 2005;58:840–6.ArticlePubMed
- 7.Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol 2011;69:292–302.ArticlePubMedPMC
- 8.Filippi M, Rocca MA, Ciccarelli O, De Stefano N, Evangelou N, Kappos L, et al. MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines. Lancet Neurol 2016;15:292 –303..Article
- 9.Sombekke MH, Wattjes MP, Balk LJ, Nielson JM, Vrenken H, Uitdehaag BM, et al. Spinal cord lesions in patients with clinically isolated syndrome: a powerful tool in diagnosis and prognosis. Neurology 2013;80:69–75.ArticlePubMed
- 10.Weier K, Mazraeh J, Naegelin Y, Thoeni A, Hirsch JG, Fabbro T, et al. Biplanar MRI for the assessment of the spinal cord in multiple sclerosis. Mult Scler 2012;18:1560–9.ArticlePubMed
- 11.Okuda DT, Mowry EM, Beheshtian A, Waubant E, Baranzini SE, Goodin DS, et al. Incidental MRI anomalies suggestive of multiple sclerosis: the radiologically isolated syndrome. Neurology 2009;72:800–5..Article
- 12.Horowitz AL, Kaplan RD, Grewe G, White RT, Salberg LM. The ovoid lesion: a new MR observation in patients with multiple sclerosis. AJNR Am J Neuroradiol. 1989;10:303–5.PubMedPMC
- 13.Grossman RI, Barkhof F, Filippi M. Assessment of spinal cord damage in MS using MRI. J Neurol Sci. 2000;15:172 Suppl.1:S36–9.Article
- 14.Lucchinetti CF, Popescu BF, Bunyan RF, Moll NM, Roemer SF, Lassmann H, et al. Inflammatory cortical demyelination in early multiple sclerosis. N Engl J Med 2011;365:2188–97.ArticlePubMedPMC
- 15.Calabrese M, De Stefano N, Atzori M, Bernardi V, Mattisi I, Barachino L, et al. Detection of cortical inflammatory lesions by double inversion recovery magnetic resonance imaging in patients with multiple sclerosis. Arch Neurol 2007;64:1416–22.ArticlePubMed
- 16.Filippi M, Rocca MA, Calabrese M, Sormani MP, Rinaldi F, Perini P, et al. Intracortical lesions: relevance for new MRI diagnostic criteria for multiple sclerosis. Neurology 2010;75:1988–94.ArticlePubMed
- 17.Kilsdonk ID, Lopez-Soriano A, Kuijer JP, de Graaf WL, Castelijns JA, Polman CH, et al. Morphological features of MS lesions on FLAIR* at 7 T and their relation to patient characteristics. J Neurol 2014;261:1356–64.ArticlePubMed
- 18.Tallantyre EC, Dixon JE, Donaldson I, Owens T, Morgan PS, Morris PG, et al. Ultra-high-field imaging distinguishes MS lesions from asymptomatic white matter lesions. Neurology 2011;76:534–9.ArticlePubMedPMC
- 19.Charil A, Yousry TA, Rovaris M, Barkhof F, De Stefano N, Fazekas F, et al. MRI and the diagnosis of multiple sclerosis: expanding the concept of “no better explanation”. Lancet Neurol 2006;5:841–52.ArticlePubMed
- 20.Kim SH, Kim W, Li XF, Jung IJ, Kim HJ. Does interferon beta treatment exacerbate neuromyelitis optica spectrum disorder? Mult Scler 2012;18:1480–3.ArticlePubMed
- 21.Wingerchuk DM, Banwell B, Bennett JL, Cabre P, Carroll W, Chitnis T, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015;85:177–89.ArticlePubMedPMC
- 22.Weisfeld-Adams JD, Katz Sand IB, Honce JM, Lublin FD. Differential diagnosis of Mendelian and mitochondrial disorders in patients with suspected multiple sclerosis. Brain 2015;138:517–39.ArticlePubMedPMC
- 23.Pfeffer G, Burke A, Yu-Wai-Man P, Compston DA, Chinnery PF. Clinical features of MS associated with Leber hereditary optic neuropathy mtDNA mutations. Neurology 2013;81:2073–81.ArticlePubMedPMC
- 24.Rovaris M, Gambini A, Gallo A, Falini A, Ghezzi A, Benedetti B, et al. Axonal injury in early multiple sclerosis is irreversible and independent of the short-term disease evolution. Neurology 2005;65:1626–30.ArticlePubMed
- 25.Filippi M, Rovaris M, Inglese M, Barkhof F, De Stefano N, Smith S, et al. Interferon beta-1a for brain tissue loss in patients at presentation with syndromes suggestive of multiple sclerosis: a randomised, double-blind, placebo-controlled trial. Lancet 2004;364:1489–96.ArticlePubMed
- 26.Baysal Kıraç L, Ekmekçi Ö, Yüceyar N, Sağduyu Kocaman A. Assessment of early cognitive impairment in patients with clinically isolated syndromes and multiple sclerosis. Behav Neurol 2014;2014:637694.ArticlePubMedPMC
- 27.Filippi M, Horsfield MA, Morrissey SP, MacManus DG, Rudge P, McDonald WI, et al. Quantitative brain MRI lesion load predicts the course of clinically isolated syndromes suggestive of multiple sclerosis. Neurology 1994;44:635–41.ArticlePubMed
- 28.Jacobs LD, Beck RW, Simon JH, Kinkel RP, Brownscheidle CM, Murray TJ, et al. Intramuscular interferon beta-1a therapy initiated during a first demyelinating event in multiple sclerosis CHAMPS Study Group. N Engl J Med 2000;343:898–904.ArticlePubMed
- 29.Kinkel RP, Dontchev M, Kollman C, Skaramagas TT, O'Connor PW, Simon JH. Association between immediate initiation of intramuscular interferon beta-1a at the time of a clinically isolated syndrome and long-term outcomes: a 10-year follow-up of the Controlled High-Risk Avonex Multiple Sclerosis Prevention Study in Ongoing Neurological Surveillance. Arch Neurol 2012;69:183–90.ArticlePubMed
- 30.Comi G, Filippi M, Barkhof F, Durelli L, Edan G, Fernández O, et al. Effect of early interferon treatment on conversion to definite multiple sclerosis: a randomised study. Lancet 2001;357:1576–82.ArticlePubMed
- 31.Comi G, Martinelli V, Rodegher M, Moiola L, Bajenaru O, Carra A, et al. Effect of glatiramer acetate on conversion to clinically definite multiple sclerosis in patients with clinically isolated syndrome (PreCISe study): a randomised, double-blind, placebo-controlled trial. Lancet 2009;374:1503–11.ArticlePubMed
- 32.Kappos L, Polman CH, Freedman MS, Edan G, Hartung HP, Miller DH, et al. Treatment with interferon beta-1b delays conversion to clinically definite and McDonald MS in patients with clinically isolated syndromes. Neurology 2006;67:1242–9.ArticlePubMed
- 33.Kappos L, Edan G, Freedman MS, Montalbán X, Hartung HP, Hemmer B, et al. The 11-year long-term follow-up study from the randomized BENEFIT CIS trial. Neurology 2016;87:978–87.ArticlePubMedPMC
- 34.Miller AE, Wolinsky JS, Kappos L, Comi G, Freedman MS, Olsson TP, et al. Oral teriflunomide for patients with a first clinical episode suggestive of multiple sclerosis (TOPIC): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol 2014;13:977–86.ArticlePubMed
- 35.Kavaliunas A, Manouchehrinia A, Stawiarz L, Ramanujam R, Agholme J, Hedström AK, et al. Importance of early treatment initiation in the clinical course of multiple sclerosis. Mult Scler 2016.Article
- 36.Hohlfeld R. & Wekerle, H. Autoimmune concepts of multiple sclerosis as a basis for selective immunotherapy: from pipe dreams to (therapeutic) pipelines. Proc Natl Acad. Sci USA 2004;101(Suppl 2):14599–606.
- 37.Ransohoff RM, Hafler DA, Lucchinetti CF. Multiple sclerosis-a quiet revolution. Nat Rev Neurol 2015;11:134–42.
- 38.Lassmann H, van Horssen J, Mahad D. Progressive multiple sclerosis: pathology and pathogenesis. Nat Rev Neurol 2012;8:647–56.ArticlePubMed
References
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader ePub Link
ePub Link Cite
Cite
