 KOSIN UNIVERSITY COLLEGE OF MEDICINE
KOSIN UNIVERSITY COLLEGE OF MEDICINE
Articles
- Page Path
- HOME > Kosin Med J > Volume 33(3); 2018 > Article
-
Case Report
Common Hepatic Artery Originating from Left Gastric Artery: A Rare Variant Encountered in Gastric Cancer Surgery - Chang In Choi, Tae Yong Jeon
-
Kosin Medical Journal 2018;33(3):463-467.
DOI: https://doi.org/10.7180/kmj.2018.33.3.463
Published online: December 31, 2018
Gastrointestinal Division, Department of Surgery, Pusan National University Hospital, Busan, Korea.
- Corresponding Author: Tae Yong Jeon, Department of Surgery, Pusan National University Hospital 179, Gudeokro, Seogu, Busan 49241, Korea. Tel: +82-51-240-7238, Fax: +82-51-247-1365, 111160@pusan.ac.kr
• Received: September 29, 2017 • Revised: November 10, 2017 • Accepted: November 20, 2017
Copyright © 2018 Kosin University College of Medicine
Articles published in Kosin Medical Journal are open-access, distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 859 Views
- 0 Download
Abstract
- The hepatic artery can have numerous variations. However, a common hepatic artery originating from the left gastric artery and the entire hepatic blood supply furnished by the left gastric artery is an extremely rare anomaly. We encountered this anomaly in a patient with advanced gastric cancer. A surgeon should recognize this image appearance and identify the anomaly. Without knowledge of this anomaly and given the strategy for extensive lesser sac dissection generally employed during gastric cancer surgery, a surgeon could easily inadvertently divide this vessel, resulting in critical liver damage. We report a case of common hepatic artery originating from left gastric artery and review of the literatures.
- A 55-year-old man was evaluated for dyspepsia and 5 kg weight loss over 3 months. Laboratory testing showed a decreased red blood count (3.9×106/µL), hemoglobin (12.1 g/dL), and hematocrit (37.2 %). Tumor markers including CEA (3.2 ng/ml) and CA 19-9 (26.4 U/ml) revealed no abnormalities. Esophagogastroduodenoscopy demonstrated an ulcerative lesion from the prepylorus to the angle of the stomach. Endoscopic biopsy revealed moderately differentiated adenocarcinoma. Abdominal computed tomography (CT) showed perigastric fat infiltration with lymphadenopathy at the left gastric, common hepatic, and hepatoduodenal ligament lymph node. There is only the splenic artery present along the upper border of pancreas. Common hepatic artery runs toward hepatic hilum along the lower border of left lobe (Fig. 1A, B).
- After laparotomy, the greater curvature was freed after ligation, and division of the vessels with lymph node dissection, and then the duodenum was transected. During dissection from the left edge of the hepatoduodenal ligament towards the esophagus, a thick cord-like structure was found in the lesser omentum plane. The common hepatic artery, which runs transversely in parallel with the pancreatic parenchyma, was not found on the upper border of the pancreas. The number 7, 8, and 9 lymph node dissection with vessel preservation was performed carefully. The common hepatic artery had an anomalous origin, the left gastric artery arose from the celiac trunk, two accessary arteries were branched to the lesser curvature, and then it ran toward the hepatic hilum along the lower border of the left lobe (Fig. 2). A distal gastrectomy with Roux-en Y reconstruction was performed. Pathologic findings showed T4aN3M0 and Stage IIIc based on the 7th edition of American Joint Committee on Cancer. The postoperative course of the patient was uneventful and he was discharged on the 9th postoperative day. Multi-dimensional abdominal computed tomography (MDCT) was performed 1 year after the operation, as a routine follow up schedule, and a reconstructed angiographic image showed that the common hepatic artery originated from the left gastric artery (Fig. 3).
CASE
- It is well known that the hepatic artery has numerous variations. Variations of the hepatic artery have been reported on many occasions, including in the reports by Adachi in 1928 and Michels in 1955.56 However, the common hepatic artery originating from the left gastric artery has been rarely reported, and this paper reported the first intraoperative finding.234 In the study by Song, this anomaly was found in eight (0.16%) of 4939 patients.4 In the study by Michels, this anomaly was found in only one (0.5%) of 200 dissected cadaveric specimens.6
- Resection of the accessory artery or replacing the left hepatic artery arising from the left gastric artery, during gastrectomy, may cause transient liver dysfunction, usually normalized within 7 days after operation.7 Therefore, a gastric surgeon does not usually consider hepatic artery anatomic variations. However, without knowledge of this anomaly, given the strategy of extensive lesser sac dissection generally employed during gastric cancer surgery, an inadvertent division of this vessel could result in critical liver damage. Thus, the surgeon drew attention to this anatomic variation of the origin of the hepatic artery, ensuring that no damage would occur during gastric surgery. The intraoperative photography of common hepatic artery originating from left gastric artery has never been reported, therefore, this image appearance can be helpful for surgeons during upper gastrointestinal tract and hepatobiliary surgery.
- Abdominal computed tomography is routinely performed for patients with gastric cancer to assess local invasion and distant metastasis. With the technological advancement of multi detector computed tomography (MDCT) technology, vascular anatomic reformation can now be easily delineated. Rapid volumetric acquisition of thin-slice high resolution images of the abdominal arteries with the help of MDCT allows reconstructions to be created, providing the surgeon with patient's arterial anatomy.8 In patients with gastric cancer, preoperative reformation vascular anatomy using an MDCT scan may provide useful information to the surgeon, bearing in mind this anatomical variation discovered during gastric surgery.
DISCUSSION
Acknowledgments
Acknowledgement
- 1. Noussios G, Dimitriou I, Chatzis I, Katsourakis A. The main anatomic variations of the hepatic artery and their importance in surgical practice: review of the literature. J Clin Med Res 2017;9:248–252.ArticlePubMedPMC
- 2. Uva P, Arvelakis A, Rodriguez-Laiz G, Lerner S, Emre S, Gondolesi G. Common hepatic artery arising from the left gastric artery: a rare anatomic variation identified on a cadaveric liver donor. Surg Radiol Anat 2007;29:93–95.ArticlePubMed
- 3. Okada Y, Nishi N, Matsuo Y, Watadani T, Kimura F. The common hepatic artery arising from the left gastric artery. Surg Radiol Anat 2010;32:703–705.ArticlePubMed
- 4. Song SY, Chung JW, Yin YH, Jae HJ, Kim HC, Jeon UB, et al. Celiac axis and common hepatic artery variations in 5002 patients: systematic analysis with spiral CT and DSA. Radiology 2010;255:278–288.ArticlePubMed
- 5. Adachi B. Das Arteriensystem der Japaner. Vol 2. verlag der Kaiserlich-Japanishen Universitat zu Kyoto; 1928. p. 20–46.
- 6. Michels NA. Newer anatomy of the liver and its variant blood supply and collateral circulation. Am J Surg 1966;112:337–347.ArticlePubMed
- 7. Okano S, Sawai K, Taniguchi H, Takahashi T. Aberrant left hepatic artery arising from the left gastric artery and liver function after radical gastrectomy for gastric cancer. World J Surg 1993;17:70–73.ArticlePubMed
- 8. Thangarajah A, Parthasarathy R. Celiac Axis, common hepatic and hepatic artery variants as evidenced on MDCT angiography in Sourth Indian population. J Clin Diagn Res 2016;10:TC01–TC05.
References
Fig. 1
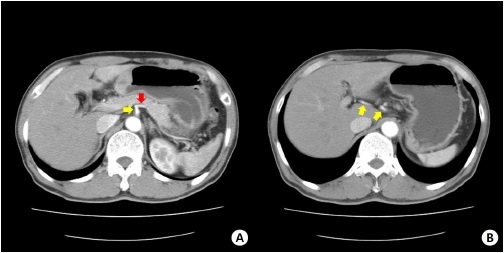
Preoperative abdominal computed tomography scan. (A) There is only the splenic artery present along the upper border of pancreas (red arrow). Celiac trunk was presented with yellow arrow. (B) Common hepatic artery runs toward hepatic hilum along the lower border of left lobe (yellow arrow).
Fig. 2

Intraoperative finding. The left gastric artery (LGA) is arising from celiac trunk, two accessary arteries were branched to lesser curvature (yellow arrows) and then, it run toward hepatic hilum along the lower border of left lobe (black arrow).
Fig. 3

CT angiography. The left gastric artery (LGA) originates from the celiac trunk. The left gastric artery angulated and run toward hepatic hilum and branches into left hepatic artery (LHA), the right hepatic artery (RHA) and gastroduodenal artery (GDA). There is no communication between hepatic artery and superior mesenteric artery (SMA). Black arrow; common hepatic artery, gray arrow; branches of LGA, white arrow; GDA
Figure & Data
References
Citations
Citations to this article as recorded by 
 PubReader
PubReader Cite
Cite


